
|
|
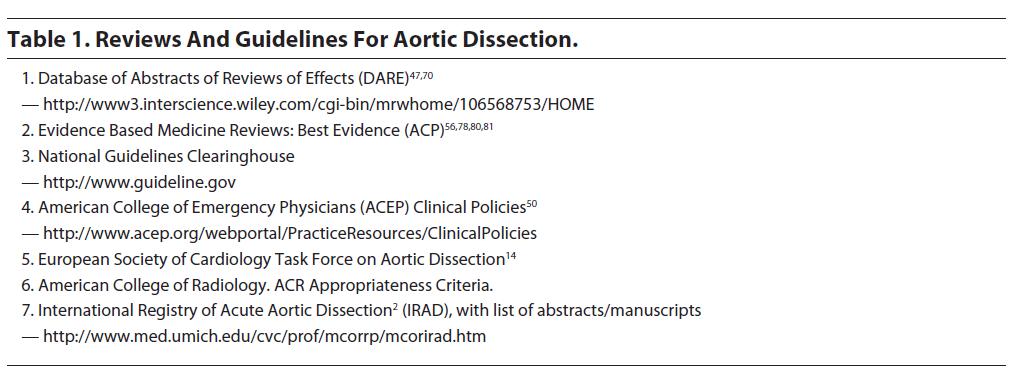
An extensive literature search was performed using MEDLINE® from 1966 to present. Clinical policies and guidelines from major societies were also reviewed for recommendations and guidelines pertaining to this topic. The key guidelines and data reviewed in the literature that the emergency medicine physician should be familiar with are listed in Table 1.
 |
An abdominal aortic aneurysm is a focal dilatation of the 3 layers of the abdominal aorta vessel wall of at least 50% more than the expected normal diameter (or proximal segment) of the aorta.7 Aortic diameter may vary according to age, sex, race, height, weight, body surface area, and baseline blood pressure.7 Risk factors for the development of AAA are provided in Table 2.8-10

Aortic dilatation and aneurysms occur in a minority of patients with Turner syndrome and can result in premature death. In a review of 67 cases of Turner syndrome and aortic dilatation, 3 patients (4%) had severe descending aortic dilatation.10 Aortic aneurysms occur in 10-48% of patients with Takayasu's arteritis, with descending thoracic and thoracoabdominal aortic aneurysms being more common than proximal aortic and isolated infrarenal aneurysms.19 Autosomal dominant polycystic kidney disease may be associated with ruptured AAAs.20
Some studies have asserted that the size of an aneurysm correlates with its rate of growth over time. However, a large, population-based cohort study of 176 patients in Rochester, Minnesota found no correlation between aneurysm size and growth rate.21 The vast majority of aneurysms expand at a rate of 0.2-0.3 cm/year, with only 20% of aneurysms expanding faster than 0.4 cm/year.21,22 In general, the larger the aneurysm, the greater the risk of rupture. (Table 3) Additional risk factors for rupture include hypertension, underlying chronic obstructive pulmonary disease (COPD), diameter exceeding 6 cm in men and 5 cm in women, local outpouchings, termed "blebs" or "blisters," of the aneurysm wall, eccentric or saccular aneurysms, rapid AAA expansion >1 cm per year, a familial history of AAAs in other first-degree relatives, and an increase in diameter over 5 mm in any 6-month period (regardless of initial or baseline size).23-28 The diameter ratio of the aneurysmal segment to the proximal normal aorta is considered by many surgeons as potentially important in determining rupture risk, but this concept has yet to be validated.23

Retroperitoneal AAA rupture is more likely to be seen in patients arriving at hospitals alive, while intraperitoneal rupture is usually rapidly fatal.5 Similar to aortic dissection, mortality is directly related to the timeliness of diagnosis before rupture and definitive repair. Delays in diagnosis are due to nonspecific presenting clinical symptoms.1,6
The aortic wall consists of 3 basic layers: the inner intima, middle media, and outer adventitia. (Figure 1) A specific arrangement of structural proteins within these layers provides strength and elasticity. With increasing age, atherosclerosis, cystic medial necrosis, vasculitis, and more rare infectious disease states or congenital abnormalities, the composition of the extracellular matrix proteins in the media changes.7 This leads to weakening of the aorta wall. If uncorrected, irreversible dilatation of the aortic wall due to the forces of systolic pressure (eg, the rate of rise of systolic blood pressure) leads to progressive dilatation and rupture.7

Abdominal aortic aneurysms are usually infrarenal.29 This segment is believed to be more prone to developing aneurysms for several reasons. First, this segment expands the most during systole and contracts the most during diastole.7 Secondly, the wall of this part of the aorta is thinner and has fewer smooth muscle cells and adventitial vasa vasora than suprarenal and thoracic aorta.30 Finally, this area is more prone to atherosclerosis, a proposed nidus for aneurysmal dilatation.31 Isolated suprarenal AAAs are uncommon; aneurysms in this location tend to be extensions of either infrarenal or thoracic aneurysms.32
Mycotic aneurysms and pseudoaneurysms are named for their mushroom-like appearance. Mycotic aneurysms are focal aortic dilatations from infection (eg, hematogenous spread of microorganisms) and inflammation that results in weakening of the aortic wall.8 They are typically infrarenal in location and occur much less frequently than aneurysms from underlying atherosclerotic lesions, but they are more likely to expand rapidly and rupture without surgical intervention.8 Bacterial spread to the aorta may occur via several mechanisms:
Prior to the advent of antibiotics, endocarditis from Streptococcus pyogenes was the most common cause of mycotic aneurysms. Today, small case series suggest that Salmonella has emerged as the most common bacterial cause of mycotic aneurysms, with Streptococcus and Staphylococcus being less common.33-35 Salmonella preferentially affects diseased tissues, especially atherosclerotic vascular endothelium.36 Clostridium septicum has been associated with gas in the aortic wall (a rare finding) and is associated with occult gastrointestinal hemorrhage and hematologic malignancy.37 In patients with a known aortic aneurysm and a fever of unknown etiology, bacterial aortitis should be rapidly excluded.38
These aneurysms were first described in 1972 and are defined as an aortic wall aneurysm resulting from chronic inflammation associated with dense perianeurysmal fibrosis.39 Approximately 3% of AAAs are known to be inflammatory (occurring more frequently in men than women, with ratios in studies ranging from 6:1 to 30:1).39 The mean age in this population is between 62-68 years.39 Smoking, possibly viruses, familial tendency, rheumatic fever, rheumatoid disease, seronegative spondyloarthropathic disorders (ankylosing spondylitis, inflammatory bowel disease, and psoriasis), Behcet's syndrome, giant-cell aortitis, and Takayasu's aortitis are associated with inflammatory aortic
aneurysms.19,39,40
Abdominal aortic aneurysm is the thirteenth leading cause of death in the United States and is responsible for 0.8% of all deaths — AAA is the tenth leading cause of death in older men.42 The incidence of AAA is increasing as the population ages, with approximately 15,000 people dying from AAA each year in the United States (8700 of these deaths occurring from acute rupture).4,41 The prevalence of AAAs in individuals over 50 years old is 1-5%.41 There is a higher incidence in men (11.3/100,000) than women (3/100,000).43 A retrospective study of 957 patients suggested that spontaneous AAA rupture occurs more commonly within the first 3 hours of awakening, in the winter, and on Monday mornings.44
Diagnosing AAA poses unique challenges, since the presence and expansion of AAAs typically constitute a silent disease, with rupture occurring quickly and without a specific syndrome.1 Patients with AAA may present with a myriad of complaints and symptoms caused by rapid expansion of the aneurysm, branch vessel ischemia or thrombosis, and frank rupture.5 One observational study of 125 patients with suspected AAA who presented with the combination of either abdominal, flank, or back pain and syncope found that 27 patients had AAAs.1
AAA appears in the differential diagnosis of a wide range of disorders, including acute myocardial infarction, cholecystitis, pancreatitis, peptic ulcer disease or gastritis, gastrointestinal hemorrhage, idiopathic back pain or radiculopathy, nephrolithiasis, and diverticulitis. In addition, the clinical diagnosis of symptomatic AAA by physical exam alone is notoriously unreliable.5 A review of the efficacy of the abdominal examination found that only 39% of AAAs were palpated by clinicians, with an overall positive predictive value of only 43%.45
Similar to thoracic aortic dissection, up to 30% of patients with AAA are initially misdiagnosed. In a retrospective review of 152 patients with a ruptured AAA that was missed, the most common misdiagnoses were renal colic (24%), diverticulitis (13%), and gastrointestinal bleeding (13%).5,46 The ACEP clinical policy, "Critical Issues for the Initial Evaluation and Management of Patients Presenting with a Chief Complaint of Nontraumatic Acute Abdominal Pain," specifically identifies the atypical presentations of AAA, especially in the elderly, in an attempt to alert the clinician to the challenge posed by these patients and to help emergency physicians avoid misdiagnoses.42
Suspect ruptured AAA in patients with the sudden onset of abdominal pain (possibly radiating into the back) and
hypotension. In these cases, quickly transport the patient to a facility with in-house vascular surgery.47 EMS providers may offer the only historical clues to a ruptured aneurysm as the cause of sudden shock or cardiac arrest.47
Hypotensive patients and those suspected of AAA rupture should have 2 large-bore IVs and be placed on 100% oxygen by a nonrebreather facemask.
Initial stabilization includes large-bore IV access or central venous access to allow for fluid resuscitation and blood transfusion. In cases of profound hemorrhagic shock, type O-negative blood (or possibly O-positive in men or children who are not of child-bearing age) may be emergently infused to maintain oxygenation until type-specific blood is available. Vascular surgery consultation should be initiated, with simultaneous preoperative testing and diagnostic imaging. Intubation and ventilatory assistance may be required in shock states. An ECG evaluating for signs of myocardial ischemia and a chest radiograph looking for signs of congestive heart failure, active pulmonary infection, or chronic obstructive pulmonary disease are important in risk stratifying patients and preoperative planning. Early notification of an appropriately trained surgeon and the operating room staff is key to patient survival.
Classically, patients with AAA present with back, abdominal, chest, flank, buttock, leg, groin, or scrotal pain. Back pain in the stable patient may be associated with simple aneurysmal dilation or rupture into the retroperitoneum with tamponade, whereas back pain in the unstable patient is associated with free retroperitoneal or peritoneal rupture.
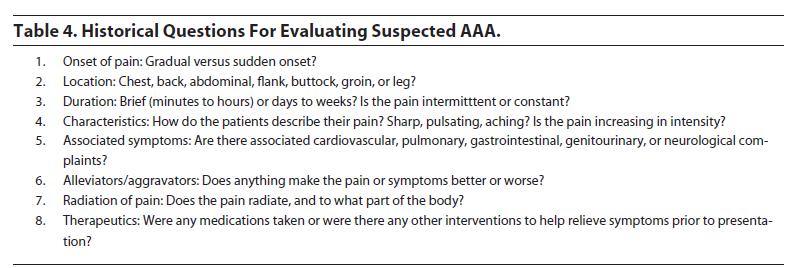
Table 4 offers a list of key questions physicians should ask to evaluate for possible AAA. The review of systems should focus on associated symptoms that can provide clues to the diagnosis. Clinicians should also focus on cardiopulmonary, gastrointestinal, and neurological symptoms, including chest pain, dyspnea, hematemesis, and rectal bleeding, as well as any mention of a syncopal episode or focal neurological complaints of weakness or numbness in the extremities. Nausea, vomiting, and oliguria or anuria may occur, due to compression of bowel loops or ureters.5Hematuria may also be present, with 1retrospective study reporting an 87% incidence of hematuria among patients with ruptured AAA50 — this may lead to the misdiagnosis of AAA as a kidney stone. In addition, symptoms may be present from hours to weeks before presentation, especially in those patients with inflammatory aneurysms, who may present with a primary complaint ofanorexia and weight loss over time.39
 |
Patients with abdominal aortic aneurysm may present with significantly elevated blood pressures, stable vitals signs, or in shock. Patients with a retroperitoneal rupture can be normotensive due to containment with a tamponade effect limiting the extent of bleeding.5 Tachycardia may be present from hemorrhage or a simple pain response. The presence of a fever suggests a mycotic aneurysm.51,55
Signs of congestive heart failure (especially JVD or a S3) or arrhythmias assist with preoperative risk stratification and guide initial stabilization. Palpation of the lower extremities should be performed to identify femoral extremity pulse deficits, cyanosis, and hypoperfusion. The best way to palpate the femoral pulse (especially in hypotensive patients) is by pressing deeply with 2 hands (one on top of the other) below the inguinal ligament, midway between the symphysis pubis and anterior superior iliac spine.52 The presence of any deficits may indicate acute limb ischemia and thrombosis. Inspection and auscultation of the chest is done for signs of congestive heart failure, pulmonary infection, or chronic obstructive pulmonary disease. These findings are important in risk stratifying patients and preoperative planning.
The abdominal exam focuses on palpation and auscultation to identify a pulsatile mass and/or bruit. The aortic bifurcation is at the level of the umbilicus, and an AAA can generally be palpated at or above the level of the umbilicus.49 The aneurysm may extend below the umbilicus, if it involves the iliac arteries. The right border of the aneurysm may be palpable to the right of the midline, a finding usually absent in patients with a normal or tortuous aorta.38,53 In a meta-analysis on the accuracy of the physical exam for detecting an AAA, the pooled sensitivity of abdominal palpation increases significantly with AAA diameter (p <0.001) — 29% for AAAs of 3.0 to 3.9 cm, 50% for AAAs of 4.0 to 4.9 cm, and 76% for AAAs of 5.0 cm or greater.45 The overall positive predictive value of detecting an AAA on physical exam is only 43%, with accuracy improving with increasing AAA size and smaller abdominal girth (<40 inches).45 Tenderness on exam likely indicates aneurysm expansion or rupture.54 The classic triad of hypotension, back pain, and a pulsatile abdominal mass or bruit as a presentation for a ruptured AAA is actually resent in fewer than 50% of patients.1,42 A rectal exam with gross blood or melena may indicate an aortoenteric fistula, especially in patients who have a previously diagnosed or repaired AAA.
Assess possible AAA patients for neurologic deficits that may indicate a central or peripheral ischemic event. AAA may cause ischemic myelopathy of the lumbar spine by occluding the great radicular artery of Adamkiewicz. Radicular arteries from the aorta supply segments of the spinal cord. Ischemic myelopathy of this type may present with motor and sensory leg deficits and posterior column (eg, vibration and position sense) sparing.
Draw blood for a CBC, BUN and creatinine, PT/PTT, INR, and for type and crossmatch (6-10 units for unstable patients). Other laboratory testing is based on clinical status and presentation. Cardiac enzymes may be sent to evaluate for active ischemia or infarction, while arterial blood gases, liver function testing, and blood lactate levels may be used to assess overall respiratory and metabolic status and to evaluate for possible mesenteric ischemia. One small observational study of 62 patients reported that a perioperative increase of cardiac troponin I correlated with increased postoperative death, but further study is needed to delineate the role of this biomarker in the evaluation and management of AAA.57
A urinalysis should be obtained, though clinicians are cautioned to remember that both ruptured AAA and renal colic present with back pain and hematuria. Urinalysis showing evidence of infection is an indication for administering preoperative antibiotics to decrease the potential risk of infection of the synthetic graft material used in surgical and endovascular interventions.56
Blood cultures are recommended in patients with suspected mycotic aneurysm or possible graft infection in patients who have undergone previous repair to help identify the causative agent.8 Specifically, patients with abdominal pain and/or fever with recent or previously documented Salmonella infection may have a mycotic aneurysm. Other patients in this category include those with bacteremia or significant invasive infection from both gram-positive and gram-negative bacteria (especially Streptococcus and Staphylococcus) and known risk factors for AAA. Patients with previously documented syphilis infection who are suspected of having tertiary syphilis with cardiovascular involvement should have an initial nontreponemal test (RPR or VDRL), with a fluorescent treponemal antibody absorption test (FTA-ABS) sent if the initial screen is positive.
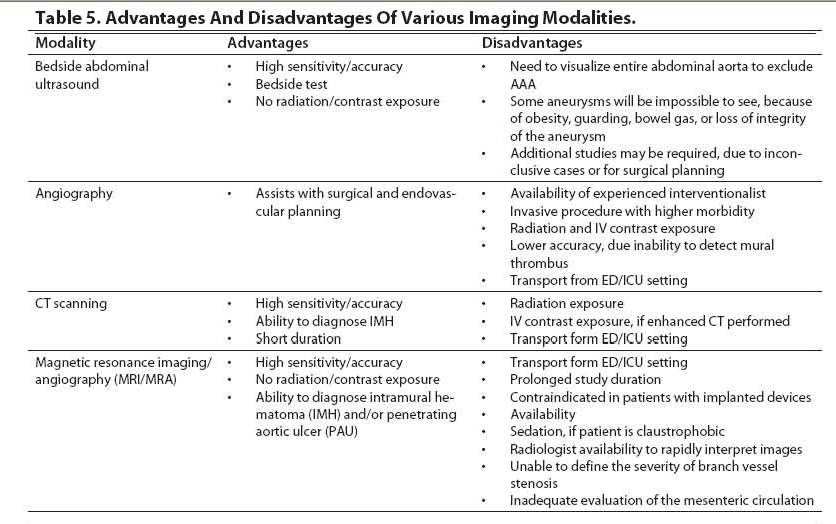
Patients with suspected AAA generally require immediate imaging. CT scanning without contrast, recommended by some as the first diagnostic test in the evaluation of a potentially ruptured AAA, may be used as a confirmatory test after ultrasound (US) has been performed, either in the ED or by radiology when the patient is stable.1,8 When there are no contraindications, contrast-enhanced CT scanning is useful in identifying the entire aorta, the retroperitoneum, and the branch and end arteries, which allows for surgical planning.8 Angiography can evaluate branch vessel involvement, but it has lower sensitivities because it only identifies the patent lumen.5 MRI has high accuracy and provides excellent anatomical detail, but MRI availability and the stability of patients often preclude its use in the emergency setting.5 (Table 5)
 |
Bedside emergency ultrasound (US) provides physicians with a tool to rapidly diagnose a potentially life-threatening process by a noninvasive, accurate, and readily available imaging modality.1 In unstable patients, it permits continued resuscitative efforts, without the need to transport patients out of the ED. If an aneurysm is found by ultrasound in an unstable patient, emergent vascular surgery consultation is warranted.60 In stable patients, bedside US permits assessment of the aorta, while also investigating other possible causes of the patient's symptoms, including cholecystitis and renal colic.5 One observational study of 125 patients with suspected AAA and either abdominal, flank, or back pain and syncope found 27 AAAs, with immediate operative management considered in 63% of the patients.1 A study from 1998 demonstrated improved outcomes and decreased time to diagnosis in patients with ruptured AAA when bedside US was used (5.4 minutes), compared to 83 minutes with traditional diagnostic modalities.59 Additionally, in this study the time to disposition for patients requiring operative intervention was decreased from 90 to 12 minutes. Multiple studies performed in the United States and internationally demonstratedthat ultrasound performed by many specialties had a 100% sensitivity for determining the size of the aorta and detecting an AAA.1,5,41,60 There have been 2 studies examining the use of ultrasound by emergency physicians; both found 100% sensitivities in the diagnosis of AAA.1,58
Nonetheless, ultrasound can be technically difficult in certain patient groups.5 Results from the above studies depend on the ability to visualize the entire abdominal aorta to determine the presence or absence of an AAA. The radiology literature has already shown that some aneurysms will be impossible to see, because of obesity, guarding, bowel gas, or loss of integrity of the aneurysm.5 A study of abdominal ultrasound in the emergency setting (on patients who had not fasted) found that a significant portion of the abdominal aorta (defined as at least one third of its length) was not visualized in up to 8% of patients, and that this was possibly related to significant bowel gas.61 A tortuous aorta may be difficult to identify and track, and isolated iliac or renal artery aneurysms may not be visualized. Off-center US beam location or measurement in the sagittal plane may underestimate the size of the aorta. Finally, US is unable to detect the presence or absence of rupture, underscoring the fact that the primary application of beside US is for determining the existence or absence of an aneurysm.5 Clinicians should also bear in mind that hydronephrosis due to ureteral obstruction from a compressing retroperitoneal hematoma may occur, complicating the picture in patients with a history suggestive of nephrolithiasis. Case-by-case judgment and maintaining a high clinical suspicion will assist physicians in ordering confirmatory studies in high-risk patients, despite an initial negative or nondiagnostic bedside US study.5
Ultrasound findings consistent with an AAA include an enlarged abdominal aorta of >3 cm (ie, a 50% increase in its normal diameter) or focal dilatation of the aorta. An intramural thrombus appears as an echoic substance within the lumen of the aorta. (Figure 2) US is insensitive for retroperitoneal bleeding from rupture, and its sensitivity in detecting extraluminal blood flow is as low as 4%.5 Free fluid in Morrison's pouch, the splenorenal space, or on the suprapubic view may be seen in patients with intraperitoneal rupture; however, most of these patients are in cardiac arrest, decreasing the clinical usefulness of this information.5 In summary, US by properly trained physicians can be used as a primary diagnostic tool in the evaluation of patients presenting with abdominal or back pain with hypotension or shock, based on its proven ability to provide a rapid diagnosis and expedite surgical consultation and management.5,60 In certain hospital settings — those without vascular, cardiopulmonary bypass, or interventionalcapabilities — early bedside diagnosis of AAA facilitates early transfer to an appropriate hospital for definitive treatment.
.
Abdominal CT scanning has a high sensitivity for detecting AAA and evaluates the entire aorta and AAA (including the presence of thrombus and visualization of the retroperitoneum).5 Disadvantages include the need for intravenous contrast in some cases, transport of potentially critically ill patients from the ED, and limited CT availability at some institutions. The most common types of CT scanners used today are the single detector-row helical CT and the 4-channel multidetector-row CT (MDCT), with the more recent addition of 8- and 16-channel MDCT. The latter modalities allow for improved spatial and temporal resolution by acquiring thinner images at faster speeds.8 Diagnosis of aortic pathology is enhanced by the ability to reconstruct these thinner images.8
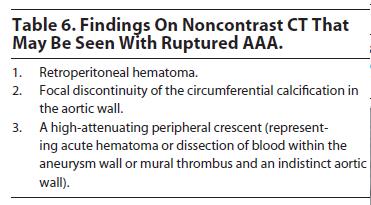
Oral contrast is not recommended, since it delays time to diagnosis, and its presence may interfere with 3-dimensional reconstruction.8 An initial study without intravenous contrast can be obtained, as this may be all that is required to diagnose an AAA.8 (Figure 3 ) Noncontrast images can also identify intramural hematomas (IMH) that, in the setting of an AAA, may indicate early or impending rupture. Table 6lists the findings associated with a ruptured AAA that may be found on noncontrast CT.8
Intravenous contrast is helpful in certain cases, especially when endovascular therapy is planned. However, IV contrast prolongs the imaging time and places patients at risk for renal failure, especially if they are already hypotensive.

 |
The routine use of MRI/MRA for patients with suspected AAA rupture is problematic, because of logistical issues and time constraints. Contrast-enhanced MRA (CEMRA) with gadolinium chelate is currently used, with studies showing that this modality correlates well with both surgical and angiography findings.62 There are 2 limitations of CEMRA in preoperative planning (for stable patients), including its inability to define the severity of branch vessel stenosis and its inadequate evaluation of the mesenteric circulation.62
Ruptured AAAs are a surgical emergency requiring aggressive stabilization and vascular surgery consultation. Hypotension is an overwhelmingly poor prognostic factor, while normotensive patients presenting with contained bleeding are the group most likely to survive emergency repair.58
In patients with symptomatic AAA and elevated blood pressures, beta-blocker therapy may be used to reduce blood pressure and stress on the arterial wall. Specific medications (Table 7) and target levels are similar to the treatment of thoracic aortic dissection. (For more, see Emergency Medicine PRACTICE, Volume 3, Number 2, Aortic Emergencies: Part I - Thoracic Dissections And Aneurysms, February 2006.) Adequate blood pressure control may require the addition of vasodilatory agents (nitroprusside) after beta-blockade has been initiated, to lower systolic or mean arterial pressures (MAP) to acceptable levels. Patients with contraindications may receive calcium channel blockers as first-line agents. However, exercise caution in choosing patients for antihypertensive therapy, as profound hypotension is a potential risk if the ruptured AAA worsens.
Prophylactic antibiotics are generally recommended in patents undergoing definitive repair and should be tailored for the common bacterial pathogens. In cases of suspected mycotic aneurysm due to Salmonella infection, researchers suggest the use of third-generation cephalosporins and fluoroquinolones (although resistance is beginning to emerge in the United States and internationally). Specific drug choice and duration of therapy may be based on cultures and sensitivities (if available), as well as infectious disease consultation.51,67 The Centers for Disease Control and Prevention guidelines (available at http:// www.cdc.gov/STD/treatment) for suspected tertiary syphilis with aortic involvement recommend using penicillin G benzathine (2.4 million units intramuscularly (IM) once a week for 3 weeks). In patients allergic to penicillin, alternative regimens include doxycycline (100 mg orally twice daily) or tetracycline (500 mg orally 4 times daily) for 28 days. For tuberculosis aortitis a regimen of 3-4 drugs is recommended, including isoniazide, rifampin, pyrazinamide, and pyridoxine for at least 2 months.68 In patients with mycotic aneurysm due to suspected Streptococcus or Staphylococcus infection, appropriate initial treatment can include nafcillin, dicloxacillin, ampicillin/sulbactam, or vancomycin in cases of suspected methicillin-resistant Staphylococcus aureus.68
Treatment of Takayasu's arteritis warrants special mention.19,39 Investigators agree that surgical intervention is necessary in these patients when they have large, complicated, symptomatic aneurysms (greater than twice the size of the normal aorta) or a rapidly expanding aneurysm.19 The appropriate use of corticosteroids preoperatively in patients presenting during an active episode remains undefined, since steroids are associated with weakening of the aneurysm wall and possibly rupture.19
 |
The first attempts at repair of AAAs occurred in the 1800s, while the first synthetic graft repair was performed by Voorhees in 1952.69 In 1958, DeBakey went on to use the first dacron graft, and graft materials have continued to evolve to this day, now including impregnated substances, such as collagen, albumin, gelatin, or specifically designed polymers to achieve leak-proof grafts.
Endovascular aneurysm repair (EVAR) began in 1991, with significant evolution in this catheter-based technology. 70 There are 3 commercially available EVAR devices in the United States at this time, with several more under evaluation in clinical trials.71 Current estimates are that 20,000 EVAR procedures take place each year in the United States, accounting for 36% of all AAA repairs.71 The first randomized study comparing conventional elective open surgical repair to EVAR was a large multicenter trial in patients with AAAs ≥5.5 cm.72 Results showed a significant survival benefit for EVAR over open repair — an in-hospital mortality of 2.1% versus 6.2%, respectively, and a 30-day mortality rate of 1.7% versus 4.7%, respectively. Similar results have been found in population-based studies in New York, with in-hospital mortality rates of 0.8% versus 4.2% in EVAR versus open repair in 2002.70 Recent results of the Dutch Randomized Endovascular Aneurysm Management (DREAM) multimember trial further add to the encouraging data — 30-day mortality rates of EVAR versus open repair were 1.2 and 4.6%, respectively, and the composite end point of operative mortality and severe complications was 4.7% versus 9.8%, respectively.70,73 One additional study is in progress in the US Department of Veterans Affairs medical system.70
The best candidates for elective, conventional open surgical repair may be younger, healthier patients, whereas older, higher-risk patients may benefit from EVAR.77 These recommendations were supported by a decision analysis model analyzing the EuroSTAR (EUROpean cobalt chromium STent with Antiproliferative for Restenosis) data.77 In general, higher-risk candidates for EVAR include patients with small body size, female sex, patients with underlying cardiac, pulmonary, or renal conditions, and patients with specific aneurysmal and underlying anatomical findings on preoperative imaging studies that indicate a high probability of procedure failure.71
Perhaps the greatest disadvantage of EVAR is the lack of long-term outcomes.70 Despite favorable early and midterm results for EVAR compared to open surgical repair, some studies have found the initial benefits for EVAR on mortality rates appear to vanish after 20 months of followup.74 EVAR is still being investigated with respect to its potential in the setting of ruptured AAA. A review of the studies and investigations pertaining to this question by the Cochrane Database of Systematic Reviews is now in progress.75
EVAR may benefit certain patients with AAA, but it does not offer patients a risk-free alternative.76 Overall, advantages include reduced perioperative morbidity, reduced length of hospital stay, and shorter recovery times, as well as the fact that EVAR represents a valid option for high-risk surgical candidates. Disadvantages include local hematomas at the catheterization site, endoleak, continued aneurysmal growth, structural failure or migration of the device, AAA rupture, and an approximate 10% risk of requiring a secondary procedure.70 Additionally, these patients need intense postoperative surveillance.70 Surveillance CT scans at 1, 6, and 12 months after implantation and annually thereafter are recommended to help prevent morbidity and mortality.71 MRI can be used in patients with renal insufficiency (especially the elderly) or in those with a contraindication to iodinated contrast.71
In 1829, Sir Astley Cooper was the first to describe a primary aortoenteric fistula, referring to this condition as a "sometimes but serious complication of an aneurysmatic aorta."77 Primary aortoenteric fistula (PAEF) is a rare cause of gastrointestinal hemorrhage, with an incidence of 0.0007/1,000,000 annually.78 The most common type of fistula, termed secondary aortoenteric fistula, usually occurs at the anastomosis site of a previous abdominal aortic aneurysm repair.77
Aortoenteric fistula should be included in the differential diagnosis in patients over the age of 50 who present with a gastrointestinal bleed, especially those with a history of aortic aneurysm and repair.78 Initial descriptions include a common triad of gastrointestinal hemorrhage, abdominal pain, and a pulsatile abdominal mass.77 The 3 classic presenting symptoms and signs — called Chiari's triad — are middle thoracic pain, a herald arterial bleed, and exsanguination after a symptom-free interval.78 In a meta-analysis of 332 patients, the time interval between the herald bleed and massive exsanguination was reported to range from hours to months; however, 30% of patients experienced a massive bleed within 6 hours of the herald bleed.77 Physicians should be aware that an initial thrombus that "plugs" the fistula as a result of local vasospasm and hypotension might be dislodged once intravenous fluids have restored the normotensive state. Close monitoring of fluid administration is warranted, as excessive fluid may actually promote fatal exsanguinations.77
Primary aortic fistula, defined as fistulas associated with a native aorta, can complicate AAA, aortitis, and trauma. In addition to the bowel, as described above, aortic fistulae have been reported involving the inferior vena cava, renal veins, and ureters.8
Acute abdominal aortic occlusion (Figure 4) is a rare vascular catastrophe that can escape initial detection, with patients often presenting with paralysis. This diagnosis should be considered when a patient without atherosclerosis presents with cold extremities and absent femoral pulses.8 In comparison to Leriche's syndrome, or chronic aortic occlusion, extensive collateral circulation is not present and, if left untreated, mortality is >75%.79 Etiologies of acute aortic occlusion include a large saddle embolism to the aortoiliac bifurcation, in situ thrombosis of an atherosclerotic aorta, sudden thrombosis of a small aortic aneurysm, or thrombosis related to a traumatic dissection.8 Contrast CT findings include the lack of blood flow in the aorta and the lack of defined collateral vessels.8 MRA should be considered in cases where iodinated contrast is contraindicated. Treatment typically is by embolectomy or bypass, if flow cannot be established endovascularly.79,80

.
Symptomatic AAAs require emergent surgical consultation, either surgical or interventional treatment, and admission to the ICU. Continued blood pressure manage ment in the ED is warranted, and completion of additional preoperative testing will assist in patient risk stratification. Patients with suspected mycotic or inflammatory aneurysms may require a multidisciplinary approach in medical management and surgical planning. Patients with Salmonella-infected aneurysms require urgent surgical resection of the infected tissue, followed by long-term antibiotic therapy, since mortality is 100% in patients treated conservatively with medical therapy alone.51,81
Patients with incidentally discovered, asymptomatic aneurysms whose symptoms and complaints are clearly unrelated to the aneurysm may be safely discharged with early outpatient surgical consultation for elective repair.49 These patients should have extensive discharge instructions regarding the need to seek medical attention immediately if abdominal, back, or flank pain develops, or if any ischemic or neurological symptoms develop.49 Betablocker therapy should be initiated to help reduce the risk of AAA expansion and rupture.82
In patients with asymptomatic aneurysms less than 5.5 cm, follow-up at least every 6 months with serial imaging by abdominal sonography, CT scanning, or MRI is generally recommended.83 (Table 8) The risk of rupture in AAAs measuring 5.5 cm or more is 10-15% per year, and it is generally recommended that these be repaired electively.69,70 Studies have found no significant benefit to early elective surgical repair in patients with aneurysms of 4.0-5.5 cm.83
As a rule of thumb, aneurysms are estimated to expand in size 10% of their diameter per year.84 Annual sonograms are recommended for any patient with an AAA of 3.0-4.0 cm, sonograms every 6 months if the AAA is 4.0-5.0 cm, and every 3 months if it is 5.0-5.5 cm.59 Surgery is also recommended if the aneurysm is >6 cm and for those with diameters between 4.5 and 5.9 cm that increase >1 cm/ year.59 A large study on the economic cost and health-related quality of life in this patient population showed that, while early surgical cost was more than ultrasonographic surveillance over a mean of 4.6 years, the early surgical group had higher scores for health perception.86
 |
Alternative approaches to slow the inflammatory process in the aorta wall have shown promising initial results.87 A nonrandomized trial in patients with small AAAs taking NSAIDs revealed a reduction in median aneurysm growth from 3.2 to 1.5 mm per year.87 Alternatively, research has detected the presence of Chlamydia pneumoniae DNA and antigen in atherosclerotic lesions from abdominal aortic aneurysms, and the presence of elevated IgG and IgA antibodies against C pneumoniae in patients with more rapid expansion rates of asymptomatic AAA.88 A randomized trial using an antichlamydial drug showed positive results in reducing aneurysm expansion in the first year, although there was no difference in the second year.89 However, researchers caution that the potential widespread use of prophylactic antibiotics could lead to high levels of resistance in other pathogens.88
Further research is focusing on reducing proteolytic activity in the aortic wall, with hopes of slowing or preventing the degradation by dominant proteinases in the aorta of all components of the extracellular matrix.84 A small, randomized clinical trial has shown promise using doxycycline, a broad-spectrum MMP inhibitor, with larger trials needed to consider this therapy in AAA. Additional genetic studies and small observation studies of cystatin C, an inhibitor of arterial wall proteinases, have been conducted. These suggest that a deficiency of this inhibitor contributes to the process of aneurysm expansion.90,91 In conclusion, pharmacotherapy for AAA is still in its infancy, but considerable progress is expected over the next few years.84
High clinical suspicion, rapid diagnosis (increasingly by physician-performed bedside ultrasound), initial stabilization, and urgent vascular surgery consultation can greatly affect short- and long-term complication and survival rates in patients with AAA. Open surgical repair continues to be the standard for ruptured AAA, and mortality rates remain high up to the present time, despite extensive improvement in surgical techniques over the past 50 years. Newer options, including endovascular aneurysm repair, show great promise. A large body of evidence documents the initial benefits of EVAR over conventional open surgical techniques in high-risk patients undergoing elective repair. Smaller studies indicate a possible role for EVAR in the emergent treatment of ruptured AAA. Long-term results are still lacking for endovascular repair, with ongoing and further prospective trials aiming to answer the key question of which method proves better in low- and high-risk patients over time. Additional research focusing on prevention of AAA, the ability to slow or possibly stop rates of aortic expansion, and close surveillance and screening for AAA may help decrease the significant morbidity and mortality of AAA in our growing elderly population.

The first presumed traumatic aortic rupture reported was from an autopsy performed by Vesalius in 1557, and over the centuries such injuries were assumed to be rare but universally fatal occurrences.92 In the era of high-speed transportation, patterns of traumatic injury changed, with aortic rupture often noted in victims of airplane crashes during World War I.92 Parmley's landmark study in 1958, examining 296 cases of blunt aortic injury among young soldiers, found that only about 15% survived long enough to get to a hospital.92,93 As cars became more widely available, autopsy studies in the 1960s showed an increasing incidence of aortic rupture (approximately 16% in motor vehicle collisions).92
The incidence of traumatic abdominal aortic rupture is extremely rare, with only 46 cases reported as of 1990.98 Original autopsy data from the landmark Parmley study in 1958 documented approximately 94% of injuries occurring in the thoracic aorta (majority at the aortic isthmus 55.6%), and only 6.4% involving the abdominal aorta.93
Blunt aortic injury (BAI) is the second most common cause of death from blunt trauma after head injury.97 Between 7500 and 8000 cases of BAI occur each year in the United States.94 An estimated 50% of patients with blunt aortic injury die rapidly at the scene of trauma, and less than 20% of patients survive the initial injury and transport to the hospital.95 These patients usually have partialthickness injuries in which the intima and media are torn, but the adventitia remains intact.92,94,96 About 50% of these aortic injuries will rupture in the first 24 hours and 80% in the first week, if they remain undiagnosed.96
Overall mortality for patients surviving BAI to hospital evaluation is approximately 31%, with thoracic aortic rupture the direct cause of death in a majority (63%) of cases.97 Meta-analysis of 1500 patients with BAI who were hemodynamically stable at the time of operation found a composite death rate of 21%, with a majority of these deaths attributable to complicatios associated with other injuries.113 The most common location of injury is the isthmus, accounting for 75-95% of cases.94,98
Penetrating trauma usually causes a rapidly fatal, fullthickness aortic injury, while blunt mechanisms, particularly sudden deceleration, may result in partial or complete tears.96 The aorta can be injured directly by displaced thoracic vertebral fractures or by bony compression of the aortic isthmus.93 Indirect forces can also result in aortic injury, including the tremendous pressure that can build up within the aorta at the moment of impact (water hammer effect), with subsequent rupture by an explosive outburst.93 Alternatively, trauma to the aorta has been described as due to the fixed nature of the descending aorta to the posterior chest wall. During deceleration, the heart and ascending aorta swing forward and tear free at the isthmus.92 The most common site for blunt aortic injury following blunt trauma is the descending aorta, just proximal to the ligamentum arteriosum, followed by the ascending aortic arch.96
The degree of aortic injury in blunt trauma is a continuum from subintimal hemorrhage to total aortic disruption.97 BAIs are classified into minor — grade 1 — and major — grades 2 and 3 —according to the underlying histological lesions.98
High-risk trauma patients require rapid transport to a trauma center with simultaneous resuscitation, as described above. No studies focusing on prehospital diagnosis of blunt aortic injury were found in a review of the literature.
A large, prospective, 50-center trial in North America — from the American Association for Surgery and Trauma — reported that a majority of patients (207 of 274) with blunt aortic injury who survived to a trauma center were stable at the time of hospital admission.97 The mechanism of injury remains the most important factor in establishing the diagnosis, with falls from >10 feet, motor vehicle collisions at speeds >30 mph (including side-impact collisions), unrestrained drivers, ejected passengers, pedestrians struck by motor vehicles, or injuries from severe crush/ pinned mechanisms all being at high risk for BAI.92,94,97,101,102 After the initial assessment and stabilization of the patient, the examination focuses on identifying signs of chest trauma that may indicate the presence of BAI.92 (Table 9)
 |
A widened mediastinum (Figure 5) on chest x-ray is the most frequently cited abnormality that suggests BAI and often drives additional diagnostic studies.103 However, this can be problematic, in that radiographic evaluation of trauma often begins with a supine PA view of the chest, which results in a magnified mediastinal image.92 To accommodate this magnification, a systematic review of 52 articles recommended that the upper limits of the mediastinum measurement be 9.68 cm on portable chest x-rays performed in the resuscitation, though this continues to be controversial.104 Current guidelines recommend that a widened mediastinum be defined as a measured width of >8 cm, a mediastinal/chest width ratio of >0.38 (measured at the level of the aortic arch), or simply the physician's impression that the mediastinum is widened.103 Table 10 lists findings on chest x-ray that indicate a possible BAI.
While chest x-ray is a good screening study, 7-30% of patients with BAI have a normal mediastinum on CXR.104 The sensitivity and specificity of a widened or abnormal mediastinum on initial chest x-ray for BAI has been reported as 85-92% and 10%, respectively.97,104,105 A recent, large prospective series of 494 patients with BAI found that only 67% of patients had a widened mediastinum on CXR, and 26% had a completely normal chest x-ray.108 Therefore, as in patients with nontraumatic presentations, definitive imaging is indicated in high-risk trauma patients.

.
 |
Bedside echocardiography using the subcostal 4-chamber view of the heart in trauma patients, which assesses for pericardial effusion, is part of the FAST exam. The American College of Surgeons' Committee on Trauma revised their Advanced Trauma Life Support® (ATLS®) course to integrate rapid ultrasound into the evolving standard of trauma care in 1997.96 While ACEP's "Clinical policy: critical issues in the evaluation of adult patients presenting to the emergency department with acute blunt abdominal trauma" recommends the FAST exam as an initial screening to detect hemoperitoneum, there is no specific mention or review of data pertaining to vascular aortic injuries.106 Transesophageal echocardiogram (TEE) is a rapid, accurate modality in diagnosing BAI, but it is relatively contraindicated in trauma patients with cervical injuries, and absolutely contraindicated in patients with esophageal injuries.96,107
With respect to BAI, angiography has been the diagnostic standard for over 40 years, but recent studies favor helical or spiral CT scanning over aortography, reporting sensitivities, specificities, and negative predictive values as high as 100% versus 92%, respectively. 92,101,103,108 (Figure 6 and Figure 7) Some investigators recommend restricting the use of angiography to trauma patients with contraindications to CT or TEE, patients with inconclusive results from other investigations, and those with suspected aortic branch involvement.96,103,109 A recent study on traumatic aortic injury using spiral CT scanning as the sole diagnostic test found that patients with positive scans could safely proceed to surgical thoracotomy without further studies; negative scans essentially "ruled out" any aortic injury, and only those patients with periaortic thoracic hematoma without a detectable aortic injury required angiography.92,109 Evidence of periaortic hematoma at the level of the diaphragm found on initial abdominal CT scanning should also prompt further imaging of the thoracic aorta for potential injury.110


In the acute management of the trauma patient, the significant limitations and contraindications for MRI/MRA preclude its routine use, and it is not recommended in the initial evaluation for BAI.
Patients with hypotension should initially be resuscitated with IV crystalloids, blood transfusions, and a cautious use of vasoactive agents (norepinephrine or phenylephrine), if needed to maintain adequate perfusion. If such is not already the case, an appropriately trained surgeon should become involved for operative treatment.
Several studies since the 1970s evaluating the use of antihypertensive agents in stable BAI have reported that initial treatment with antihypertensive medications in patients with suspected BAI may not only reduce the immediate risk of rupture, but may also allow for delayed repair in high-risk patients who have associated brain and pulmonary injuries or cardiac instability requiring stabilization.103,108 Recommended medical goals for initial management of BAI include systolic blood pressures of ≤100 mm Hg, heart rates <100 beats per minute or MAP <70, with slightly higher systolic pressures in elderly patients of 110-120 mm Hg to preserve end-organ perfusion. 108,111,112 The pharmacologic approach involves the early use of beta-blockers (eg, esmolol) and subsequent vasodilators (eg, nitroprusside) to lower dP/dT. Studies in trauma patients indicate that the use of invasive hemodynamic monitoring may be useful in guiding management and resuscitation of patients with BAI, especially in those with associated blunt cardiac and other intraabdominal injuries.103 Patients with BAI who do not undergo initial surgical or endovascular correction should be admitted to the surgical or trauma ICU for further management.111
The high mortality associated with aortic injury underscores the importance of having dedicated thoracic trauma surgeons operating on patients with BAI (or at the very least, dedicated trauma surgeons with significant experience).97,103 This should factor into decisions regarding transfer in rural areas with only Level II or Level III trauma centers. Minor (ie, grade 1) injuries are often medically managed with close follow-up, while grade 3 BAIs require immediate surgery. There is significant controversy around the treatment of grade 2 BAIs.98
Prompt surgical repair is indicated in most patients with BAI, though many factors — including injury location and comorbidities — must be taken into consideration. 103 Patients who are unstable with intraabdominal injuries that require laparotomy, patients with severe, closed head injuries, elderly patients, and those with significant comorbidities may not be able to undergo emergency surgery.103 These patients are generally medically managed in the intensive care setting, until complicating factors have resolved.103 In a large, prospective multicenter study involving 50 trauma centers in North America between 1993-1996, patients undergoing open surgical repair of thoracic aortic injuries had an overall mortality rate of 31%, and a rate of postsurgical paraplegia of 8.7%, primarily due to cross-clamping times of the aorta (≥30 minutes).97
Endoluminal stenting of BAI has shown significant promise toward minimally invasive therapy.114 Results from endovascular intervention for BAI are primarily from case series, which report varying results. There were 2 studies reporting no complications or paraplegia on follow-up of a total of 21 patients for up to 36 months.115,116 Other series, including a nonrandomized trial of endovascular versus open surgical repair (in both traumatic and nontraumatic ruptures), had significantly improved early results, but an increased trend toward higher stent-graft- related mortality, morbidity, and reintervention rates at midterm and late follow-up at 6 years.117-119 Complications included aortic ruptures, endovascular leaks, and the need for conversion to open surgical repair.
In summary, questions still remain regarding the long-term complications and the durability of stent-grafts, and further surveillance and studies are needed to define the appropriate use of this promising modality in the management of BAI.117,120
Blunt aortic injury continues to be a leading cause of death in trauma patients. Recent shifts to more noninvasive imaging have improved the ability and time to diagnose BAI in the critical "first hour" of trauma patient evaluation. Newer endovascular stent-graft techniques and improved patient selection criteria for delayed repair in the multiinjured trauma patient hold out great promise for improving patient outcomes in the future.
1. "The guy had sharp back and flank pain and, despite no blood in the urine, he seemed like every other guy I've ever seen passing a kidney stone — miserable."
2."She was 65 years old, had a history of diverticulosis, and demonstrated mild lower abdominal pain on exam. Her blood pressure was higher than previously noted with her history of hypertension, but she said she was under a lot of stress lately. She only had a low-grade temperature, was tolerating PO, and appeared stable, so I prescribed antibiotics for diverticulitis and discharged her to follow up with her primary care doctor in the next 1-2 days."
3. "I found no pulsatile mass on exam, and she said she must have eaten ‘bad leftovers.’ I gave her some Maalox® and sent her on her way with a smile on her face."
4. "I thought she might have an AAA, but our CT scanner was down for over an hour, so I just had to wait until it was fixed. By then she was hypotensive."
5. "Because of her obesity, I couldn't get a perfect look at the aorta, but what I did see looked normal. Besides, she said she was constipated and was having crampy pain that felt like gas to her."
6. "On examination I discovered a pulsatile mass that turned out to be a 5-cm abdominal aneurysm on bedside US. This did not appear to be related to her complaint of a ‘bad cold,’ so I told her to follow up with her doctor."
7. "He presented with acute paralysis of both legs. I sent him within 20 minutes to the MRI for evaluation for cord compression. His legs did seem a bit cool, but he said that he always felt cold."
8. "The patient's vital signs were normal on arrival to the trauma bay following her accident, and she seemed fine. She also had a normal chest x-ray, which ruled out an aortic injury."
9. "He was wearing his seat belt when he was T-boned at 40 mph. Air bags appeared to have helped, since he was walking at the scene. He only complained of neck, back, and mild chest pain along the site of a small bruise/abrasion where the seat belt had restrained him. The rest of his exam was normal, as were spinal and chest x-rays for any signs of injury. He was feeling better with ibuprofen and was discharged."
10. "We do not regularly see trauma patients. Her abdominal pain seemed worse than her chest pain, so I waited to get her prepped for CT scan before I called a surgeon at 2 am. Then they were backed up, so she did not get there for about another 45 minutes. We always seem to get bumped at night."
_1.JPG)

















Evidence-based medicine requires a critical appraisal of the literature based upon study methodology and number of subjects. Not all references are equally robust. The findings of a large, prospective, randomized, and blinded trial should carry more weight than a case report.
To help the reader judge the strength of each reference, pertinent information about the study, such as the type of study and the number of patients in the study, will be included in bold type following the reference, where available. In addition, the most informative references cited in the paper, as determined by the authors, will be noted by an asterisk (*) next to the number of the reference.
Kevin C Reed; Liesl A Curtis
March 1, 2006
Emergency Medicine Practice • CONTINUE READING
Access every issue, our complete clinical pathway library, and earn up to 190 CME credits with an annual subscription.
Stay current with a new Emergency Medicine Practice issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933