Table of Contents
About This Issue
When a patient arrives in the urgent care clinic with symptoms such as nonpitting edema, urticaria, pruritis, abdominal pain, and/or respiratory distress, angioedema is a primary differential diagnosis. While often localized and self-limiting, angioedema can quickly become a life-threatening emergency. Identification of the cause and thorough examination of the patient are crucial for appropriate management. In this issue, you will learn:
The distinctive presentations and mechanisms of histamine-mediated, bradykinin-mediated, and idiopathic angioedema.
How to be on guard for potentially life-threatening laryngeal swelling and/or anaphylaxis.
The signs and symptoms that should prompt emergent transfer to the emergency department.
The appropriate medications to effectively manage histamine-mediated angioedema, including epinephrine and antihistamines.
The special considerations and management approaches for pediatric patients.
Disposition decisions based on the type of angioedema, staging of the disease, and indications for observation.
CODING & CHARTING: Coding for angioedema is highly variable and dependent on the cause and patient presentation. Learn more in our monthly coding column.
- About This Issue
- Abstract
- Case Presentations
- Introduction
- Etiology and Pathophysiology
- Histamine-Mediated Angioedema
- Bradykinin-Mediated Angioedema
- Hereditary Angioedema
- Acquired Angioedema
- Angiotensin-Converting Enzyme Inhibitor-Induced Angioedema
- Other Drugs Associated With Angioedema
- Idiopathic Angioedema
- Differential Diagnosis
- Urgent Care Evaluation
- Initial Management and Stabilization
- Airway Assessment
- Anaphylaxis
- History
- Physical Examination
- Diagnostic Studies
- Imaging Studies
- Treatment
- Pharmacologic Treatment
- Pharmacologic Treatment for Histamine-Mediated Angioedema
- Epinephrine
- Antihistamines
- Corticosteroids
- Pharmacologic Treatment for Bradykinin-Mediated Angioedema
- Controversies and Cutting Edge
- Leukotriene Receptor Antagonists
- Tranexamic Acid
- Disposition
- Summary
- Time- and Cost-Effective Strategies
- Risk Management Pitfalls in Management of Angioedema in Urgent Care
- KidBits: Angioedema in Pediatric Patients
- Differential Diagnosis
- Urgent Care Management
- KidBits References
- Case Conclusions
- Coding & Charting: What You Need to Know
- Number and Complexity of Problems Addressed
- Amount and/or Complexity of Data to be Reviewed and Analyzed
- Risk of Complications and/or Morbidity or Mortality of Patient Management
- Clinical Pathways
- Clinical Pathway for Urgent Care Management of Adult Patients With Angioedema
- Clinical Pathway for Urgent Care Management of Pediatric Patients With Angioedema
- References
Abstract
Patients experiencing angioedema commonly self-direct to urgent care centers. While acute presentations are often transient and localized, angioedema is a potentially life-threatening event that can rapidly progress to acute airway compromise, anaphylaxis, or both. Urgent care clinicians must quickly recognize the clinical presentations that indicate the need for emergency intervention. This article reviews the etiology and pathophysiology of angioedema, including the distinct mechanisms of the primary forms of angioedema, and presents evidence-based recommendations for the evaluation, treatment, and disposition of patients with angioedema in the urgent care setting.
Case Presentations
- The symptoms started approximately 3 hours prior to his arrival at the clinic. He did not use his epinephrine autoinjector.
- He denies any shortness of breath.
- He states that he has a peanut allergy and has had similar reactions when he has eaten peanuts in the past, but he is certain there were no peanuts in or on his doughnut.
- Due to the risk of anaphylaxis associated with peanut allergies, the patient is prioritized for evaluation immediately after triage.
- He denies any new medications, chemical exposures, fevers, or exposure to animals or plants. He has not taken any NSAIDs and is not on an ACE inhibitor.
- His vital signs are: temperature, 36.4°C; heart rate, 76 beats/min; blood pressure, 123/84 mm Hg; respiratory rate, 14 breaths/min; and oxygen saturation, 98% on room air.
- On examination, his airway is patent. Mild symmetric swelling to the lips is noted. The oropharynx is unremarkable, and the uvula is midline and without swelling. There is a faint expiratory wheeze throughout lung fields. There is no visible rash, but dermographia is noted with a scratch test.
- You wonder how you should manage this patient...
- She states her lips felt “heavy” when she woke up around 8 hours ago. She says her lips are significantly swollen, but the swelling has neither worsened nor improved.
- She denies shortness of breath, voice change, rash, itching, or prior history of similar occurrences, as well as fever or infection, any known allergies, or significant family history. She said she has had no recent exposures, travel, or trauma.
- The patient’s past medical history includes hypertension, diabetes mellitus type 2, and hyperlipidemia. She reports that she currently takes lisinopril, metformin, and atorvastatin.
- Her vital signs are: temperature, 37°C; heart rate, 82 beats/min; blood pressure, 138/78 mm Hg; respiratory rate, 16 breaths/min; and oxygen saturation, 100% on room air.
- On examination, the patient is in no distress, but she has significant upper and lower lip swelling, with no oropharyngeal involvement. The rest of her examination is unremarkable.
- You wonder if you should administer an antihistamine...
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
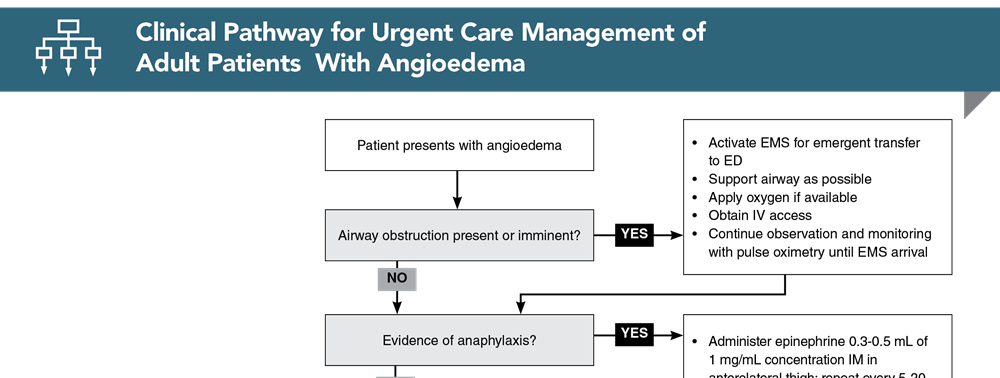
Clinical Pathway for Urgent Care Management of Adult Patients With Angioedema
Subscribe to access the complete Clinical Pathway to guide your clinical decision making.
Buy this issue and
CME test to get 4 CME credits.
Key References
Following are the most informative references cited in this paper, as determined by the authors.
1. * Macy E. Practical management of new-onset urticaria and angioedema presenting in primary care, urgent care, and the emergency department. Perm J. 2021;25(4)1-7. (Review) DOI: 10.7812/TPP/21.058
4. * Long BJ, Koyfman A, Gottlieb M. Evaluation and management of angioedema in the emergency department. West J Emerg Med. 2019;20(4):587-600. (Review) DOI: 10.5811/westjem.2019.5.42650
6. * Depetri F, Tedeschi A, Cugno M. Angioedema and emergency medicine: from pathophysiology to diagnosis and treatment. Eur J Intern Med. 2019;59:8-13. (Review) DOI: 10.1016/j.ejim.2018.09.004
12. * Bernstein JA, Cremonesi P, Hoffmann TK, et al. Angioedema in the emergency department: a practical guide to differential diagnosis and management. Int J Emerg Med. 2017;10(1):15. (Review) DOI: 10.1186/s12245-017-0141-z
19. Memon RJ, Tiwari V. Angioedema. In: StatPearls [Internet]. StatPearls Publishing. Updated August 8, 2023. Accessed February 15, 2024. (Online textbook chapter)
48. Farkas J. Angioedema. The Internet Book of Critical Care. Updated August 5, 2021. Accessed February 10, 2024. (Online textbook chapter)
Subscribe to get the full list of 50 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: histamine, bradykinin, allergy, anaphylaxis, edema, swelling, pruritis, itching, urticaria, ACE inhibitor, airway, stridor, epinephrine, cetirizine, corticosteroids









 678-366-7933
678-366-7933