

|
|
The complications of sickle cell disease (SCD) in pediatric patients are some of the more common chronic conditions that present to the emergency department. It is important that emergency clinicians understand the features of SCD, its related complications, and the associated diagnostic and therapeutic modalities to provide this patient population with the most evidenced-based and high-quality care. This review describes the acute complications and evidence-based emergent management of SCD in pediatric patients.
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
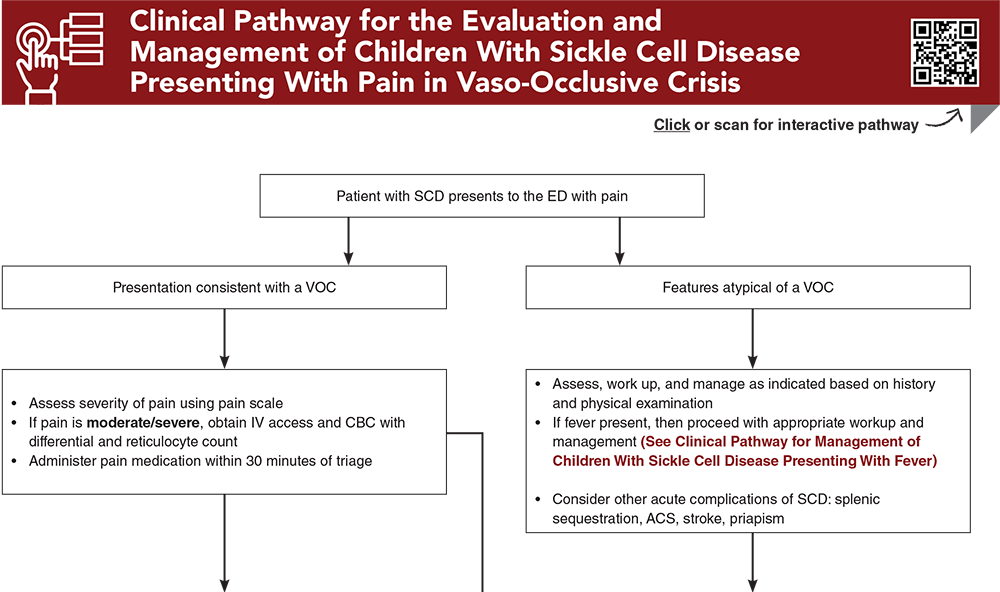
Subscribe to access the complete Clinical Pathway to guide your clinical decision making.
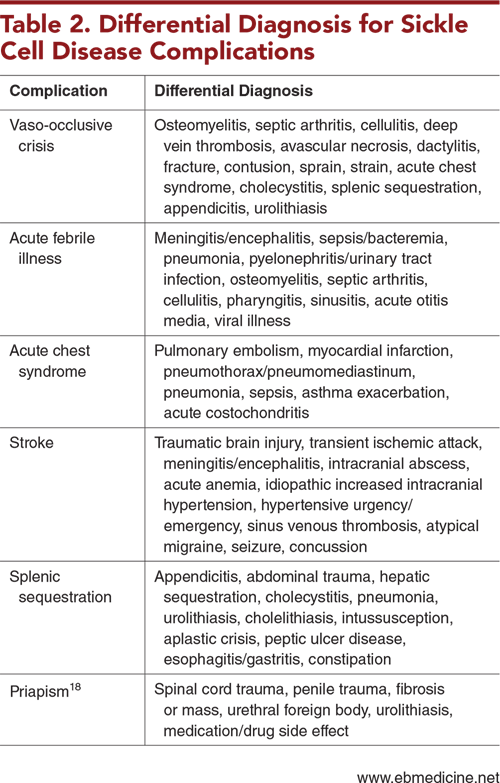
Subscribe for full access to all Tables and Figures.
Buy this issue and
Following are the most informative references cited in this paper, as determined by the authors.
1. * Piel FB, Rees DC, DeBaun MR, et al. Defining global strategies to improve outcomes in sickle cell disease: a Lancet Haematology Commission. Lancet Haematol. 2023;10(8):e633-e686. (Evidence-based expert panel report) DOI: 10.1016/S2352-3026(23)00096-0
2. * United States Centers for Disease Control and Prevention. Data & statistics on sickle cell disease. Accessed October 1, 2024. (CDC data)
4. * United States Department of Health and Human Services, National Institutes of Health, National Heart, Lung, and Blood Institute. Evidence-based management of sickle cell disease. 2014. (Expert panel report)
5. * Brandow AM, Carroll CP, Creary S, et al. American Society of Hematology 2020 guidelines for sickle cell disease: management of acute and chronic pain. Blood Adv. 2020;4(12):2656-2701. (Society guidelines) DOI: 10.1182/bloodadvances.2020001851
6. * Kavanagh PL, Hirshon JM. EDSC3: working to improve emergency department care of individuals with sickle cell disease. Ann Emerg Med. 2020;76(3S):S80-S82. (Review) DOI: 10.1016/j.annemergmed.2020.08.016
52. * DeBaun MR, Jordan LC, King AA, et al. American Society of Hematology 2020 guidelines for sickle cell disease: prevention, diagnosis, and treatment of cerebrovascular disease in children and adults. Blood Adv. 2020;4(8):1554-1588. (Expert panel review guidelines) DOI: 10.1182/asheducation-2011.1.427
Subscribe to get the full list of 103 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: pediatric sickle cell, sickle cell disease, SCD, hemoglobin, vaso-occlusive crisis, acute febrile illness, splenic sequestration, acute chest syndrome, ACS, stroke, dactylitis, priapism, sickle cell trait, SCT, ECAST, exercise collapse, hematuria, renal papillary necrosis, renal medullary carcinoma, exertional rhabdomyolysis
Kathleen M. Jackson MD, FAAP; Bradley Beamon, MD, FAAP; Erika B. Crawford, MD, FAAP, FACEP; Zachary T. Burroughs, MD, FAAP, FACEP
Stephen Rineer, MD, MS; Karen Kim Jo Yaphockun, DO
November 1, 2024
November 1, 2027 CME Information
4 AMA PRA Category 1 Credits™, 4 ACEP Category I Credits, 4 AAP Prescribed Credits, 4 AOA Category 2-B Credits.
Pediatric Emergency Medicine Practice • CONTINUE READING
Read this issue today — or unlock the entire library for a little more.
Stay current with a new Pediatric Emergency Medicine Practice issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933