

|
|
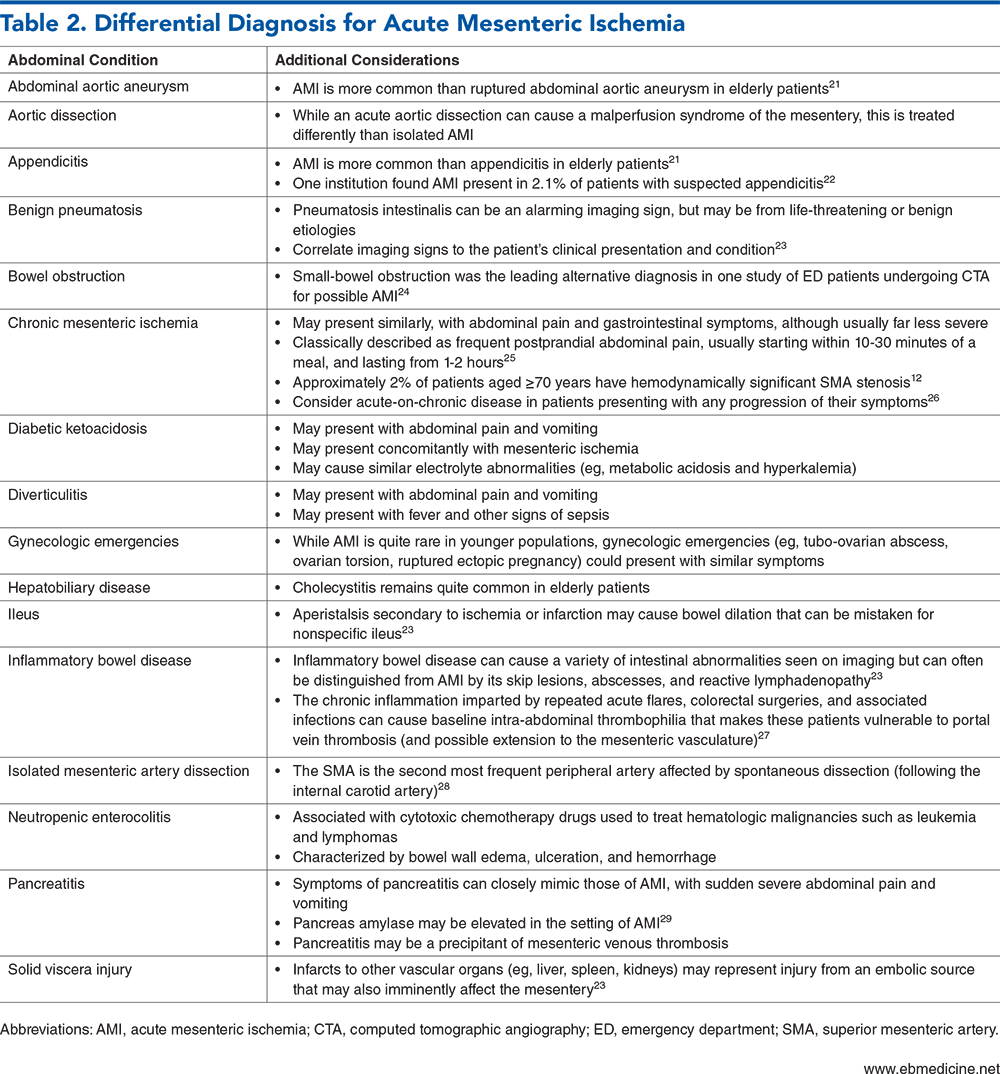
Acute mesenteric ischemia is a rare but potentially catastrophic condition, and survival is highly dependent on timely diagnosis in the emergency department. Symptoms can be both variable and subtle. Laboratory studies may be misleading and may provide either false reassurance or misdirection. This review includes evidence-based recommendations on the recognition of the 4 separate types of acute mesenteric ischemia, current guidelines on the diagnostic approach, and essential resuscitative steps that should be initiated in the emergency department.
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
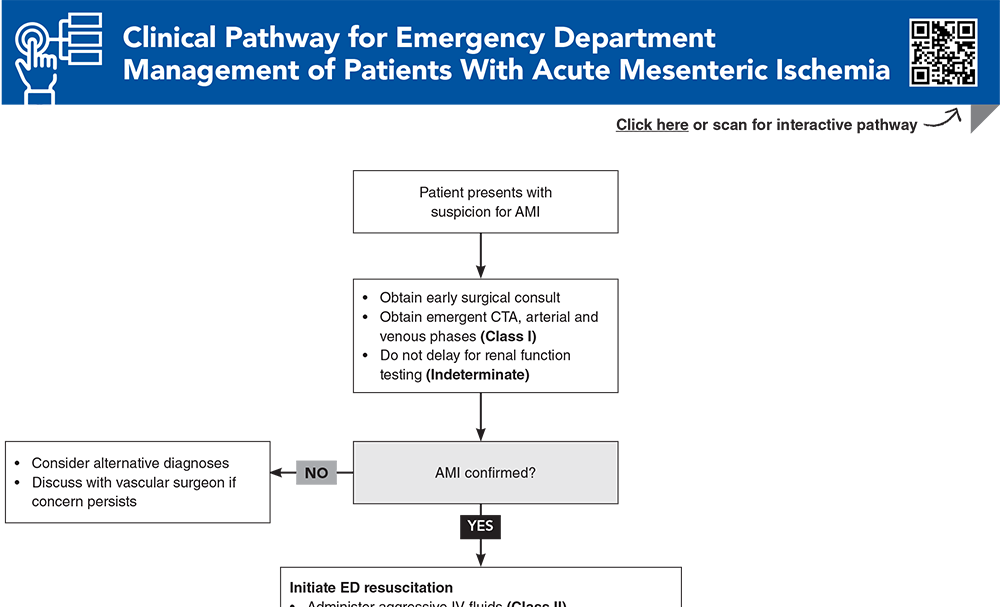
Subscribe to access the complete Clinical Pathway to guide your clinical decision making.
Subscribe for full access to all Tables and Figures.
Buy this issue and
Following are the most informative references cited in this paper, as determined by the authors.
13. * Bala M, Catena F, Kashuk J, et al. Acute mesenteric ischemia: updated guidelines of the World Society of Emergency Surgery. World J Emerg Surg. 2022;17(1):54. (Guideline) DOI: 10.1186/s13017-022-00443-x
36. * Acosta S, Salim S. Management of acute mesenteric venous thrombosis: a systematic review of contemporary studies. Scand J Surg. 2021;110(2):123-129. (Systematic review; 11 studies) DOI: 10.1177/1457496920969084
48. * Cudnik MT, Darbha S, Jones J, et al. The diagnosis of acute mesenteric ischemia: a systematic review and meta-analysis. Acad Emerg Med. 2013;20(11):1087-1100. (Systematic review; 23 studies) DOI: 10.1111/acem.12254
51. * Björck M, Koelemay M, Acosta S, et al. Editor’s choice - management of the diseases of mesenteric arteries and veins: clinical practice guidelines of the European Society of Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg. 2017;53(4):460-510. (Guideline) DOI: 10.1016/j.ejvs.2017.01.010
64. * Tilsed JV, Casamassima A, Kurihara H, et al. ESTES guidelines: acute mesenteric ischaemia. Eur J Trauma Emerg Surg. 2016;42(2):253-270. (Guideline) DOI: 10.1007/s00068-016-0634-0
72. * Ginsburg M, Obara P, Lambert DL, et al. ACR Appropriateness Criteria(®) Imaging of Mesenteric Ischemia. J Am Coll Radiol. 2018;15(11s):S332-S340. (Guideline) DOI: 10.1016/j.jacr.2018.09.018
74. * Lehtimäki TT, Kärkkäinen JM, Saari P, et al. Detecting acute mesenteric ischemia in CT of the acute abdomen is dependent on clinical suspicion: review of 95 consecutive patients. Eur J Radiol. 2015;84(12):2444-2453. (Retrospective; 95 patients) DOI: 10.1016/j.ejrad.2015.09.006
100. *Roussel A, Castier Y, Nuzzo A, et al. Revascularization of acute mesenteric ischemia after creation of a dedicated multidisciplinary center. J Vasc Surg. 2015;62(5):1251-1256. (Prospective observational; 83 patients) DOI: 10.1016/j.jvs.2015.06.204
101. *Brennan CA, Osei-Bonsu P, McClenaghan RE, et al. Vasoactive agents in acute mesenteric ischaemia in critical care. A systematic review. F1000Res. 2021;10:453. (Systematic review; 0 studies) DOI: 10.12688/f1000research.52782.2
115. *Reintam Blaser A, Starkopf J, Björck M, et al. Diagnostic accuracy of biomarkers to detect acute mesenteric ischaemia in adult patients: a systematic review and meta-analysis. World J Emerg Surg. 2023;18(1):44. (Systematic review; 75 studies) DOI: 10.1186/s13017-023-00512-9
Subscribe to get the full list of 120 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: embolism, thrombosis, bowel, infarction, ischemia, aorta, superior, inferior, nonocclusive, pancreatitis, vasoconstrictive, lactate, transmural
J. David Gatz, MD, FACEP, FAAEM; R. Gentry Wilkerson, MD, FACEP
Jennifer Beck-Esmay, MD, FACEP; Ian Storch, MD, FACEP
December 1, 2024
December 1, 2027 CME Information
4 AMA PRA Category 1 Credits™, 4 ACEP Category I Credits, 4 AAFP Prescribed Credits, 4 AOA Category 2-B Credits.
Emergency Medicine Practice • CONTINUE READING
Read this issue today — or unlock the entire library for a little more.
Stay current with a new Emergency Medicine Practice issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933