

|
|
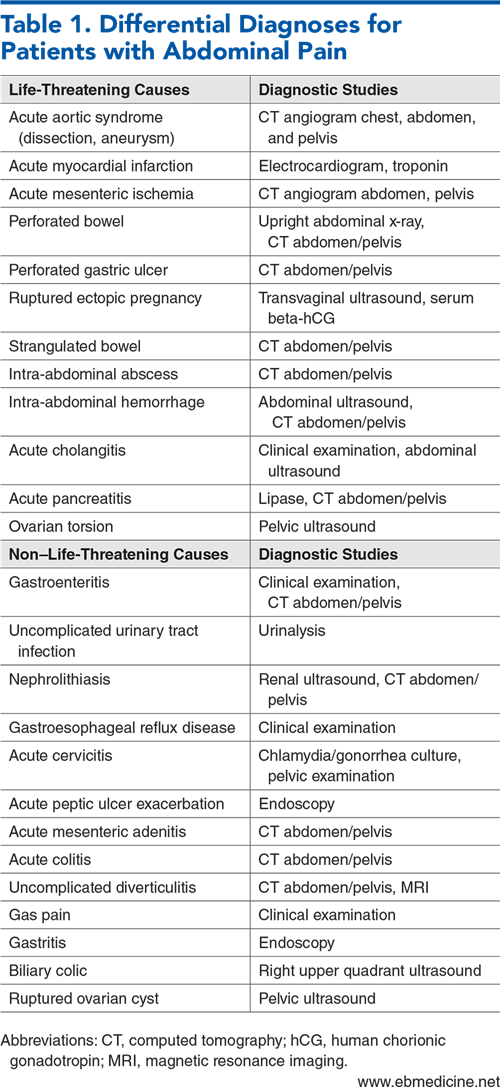
Abdominal pain is one of the most common presenting complaints to the emergency department, and appendicitis and diverticulitis are common causes. Intra-abdominal infections have historically been managed with admission to the hospital, antibiotics, and surgical interventions, and best-practice pathways are an important part of quality programs. Advances in diagnostics and management, supported with outcome data, are impacting care pathways. This review provides an update on best practices related to the management of appendicitis and diverticulitis, with the goal of improving patient care, minimizing risk, and maximizing the patient experience.
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
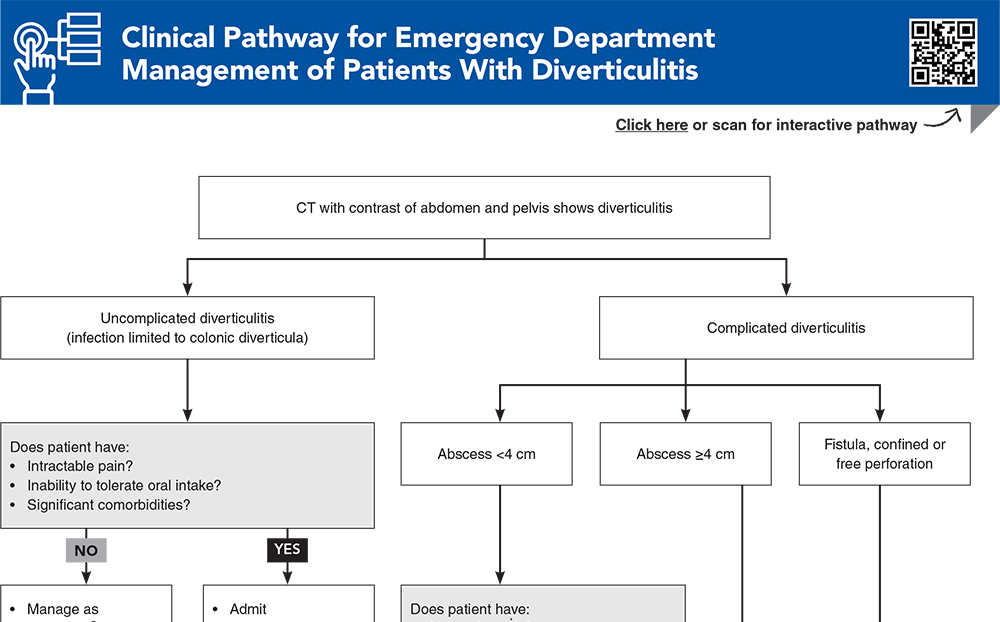
Subscribe to access the complete Clinical Pathway to guide your clinical decision making.
Subscribe for full access to all Tables and Figures.
Buy this issue and
Following are the most informative references cited in this paper, as determined by the authors.
6. * Sartelli M, Weber DG, Kluger Y, et al. 2020 update of the WSES guidelines for the management of acute colonic diverticulitis in the emergency setting. World J Emerg Surg. 2020;15(1):32. (Guidelines) DOI: 10.1186/s13017-020-00313-4
40. * Rud B, Vejborg TS, Rappeport ED, et al. Computed tomography for diagnosis of acute appendicitis in adults. Cochrane Database Syst Rev. 2019(11):CD009977. (Cochrane review; 64 studies, 10,280 patients) DOI: 10.1002/14651858.CD009977.pub2
43. * Repplinger MD, Levy JF, Peethumnongsin E, et al. Systematic review and meta-analysis of the accuracy of MRI to diagnose appendicitis in the general population. J Magn Reson Imaging. 2016;43(6):1346-1354. (Meta-analysis; 10 studies, 838 patients) DOI: 10.1002/jmri.25115
44. * D’Souza N, Hicks G, Beable R, et al. Magnetic resonance imaging (MRI) for diagnosis of acute appendicitis. Cochrane Database Syst Rev. 2021(12):CD012028. (Cochrane review; 58 studies, 7462 patients) DOI: 10.1002/14651858.CD012028.pub2
48. * Expert Panel on Gastrointestinal Imaging, Weinstein S, Kim DH, et al. ACR appropriateness criteria® left lower quadrant pain: 2023 update. J Am Coll Radiol. 2023;20(11S):S471-S480. (Guidelines) DOI: 10.1016/j.jacr.2023.08.013
53. * Lameris W, van Randen A, Bipat S, et al. Graded compression ultrasonography and computed tomography in acute colonic diverticulitis: meta-analysis of test accuracy. Eur Radiol. 2008;18(11):2498-2511. (Meta-analysis; 14 studies, 1314 patients) DOI: 10.1007/s00330-008-1018-6
64. * Fugazzola P, Ceresoli M, Coccolini F, et al. The WSES/SICG/ACOI/SICUT/ACEMC/SIFIPAC guidelines for diagnosis and treatment of acute left colonic diverticulitis in the elderly. World J Emerg Surg. 2022;17(1):5. (Guidelines) DOI: 10.1186/s13017-022-00408-0
81. * Di Saverio S, Sibilio A, Giorgini E, et al. The NOTA study (Non Operative Treatment for Acute appendicitis): prospective study on the efficacy and safety of antibiotics (amoxicillin and clavulanic acid) for treating patients with right lower quadrant abdominal pain and long-term follow-up of conservatively treated suspected appendicitis. Ann Surg. 2014;260(1):109-117. (Prospective study; 159 patients) DOI: 10.1097/SLA.0000000000000560
86. * Dichman ML, Rosenstock SJ, Shabanzadeh DM. Antibiotics for uncomplicated diverticulitis. Cochrane Database Syst Rev. 2022;6(6):CD009092. (Cochrane review; 5 studies) DOI: 10.1002/14651858.CD009092.pub3
Subscribe to get the full list of 93 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: abdominal, appendicitis, diverticulitis, abscess, peritonitis, AIR, Alvarado, ultrasound, appendicolith, antibiotics
Liza Hartofilis, MD; John K. Riggins, Jr., MD, MHA, FACEP
Marc Andrews, MD; Randy Sorge, MD, FACEP
October 1, 2024
October 1, 2027 CME Information
4 AMA PRA Category 1 Credits™, 4 ACEP Category I Credits, 4 AAFP Prescribed Credits, 4 AOA Category 2-B Credits.
Emergency Medicine Practice • CONTINUE READING
Read this issue today — or unlock the entire library for a little more.
Stay current with a new Emergency Medicine Practice issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933