

|
|
The clinical presentation for ear complaints can often overlap with other common pediatric conditions. As such, the differential diagnosis for ear complaints is broad, warranting a thorough history and targeted physical examination. Optimizing the approach for a definitive ear examination is essential when evaluating a pediatric patient with an ear concern. A systematic approach will improve the accuracy of diagnoses and the appropriateness of management. This issue provides an evidence-based approach to the diagnosis, workup, and management of common ear complaints in pediatric patients.
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
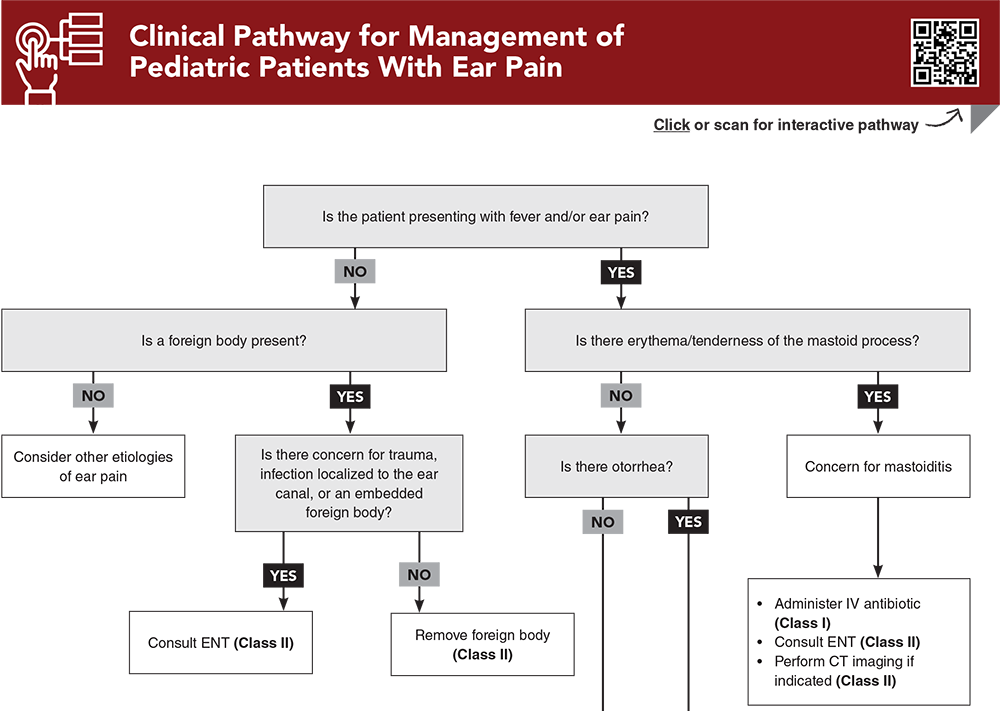
Subscribe to access the complete Clinical Pathway to guide your clinical decision making.
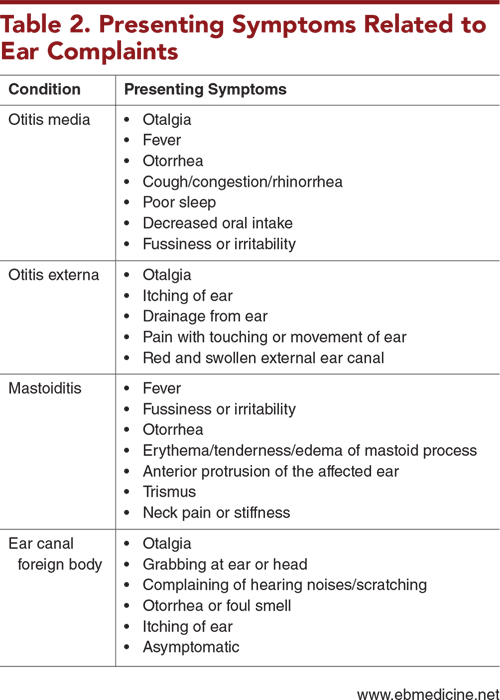
Subscribe for full access to all Tables and Figures.
Buy this issue and
Following are the most informative references cited in this paper, as determined by the authors.
4. * Lieberthal AS, Carroll AE, Chonmaitree T, et al. The diagnosis and management of acute otitis media. Pediatrics. 2013;131(3):e964-e999. (Clinical practice guidelines) DOI: 10.1542/peds.2012-3488
18. * Psarommatis IM, Voudouris C, Douros K, et al. Algorithmic management of pediatric acute mastoiditis. Int J Pediatr Otorhinolaryngol. 2012;76(6):791-796. (Retrospective; 167 patients) DOI: 10.1016/j.ijporl.2012.02.042
22. * Acevedo JL, Lander L, Shah UK, et al. Existence of important variations in the United States in the treatment of pediatric mastoiditis. Arch Otolaryngol Head Neck Surg. 2009;135(1):28-32. (Retrospective; 1049 patients) DOI: 10.1001/archoto.2008.510
28. * Prasad N, Harley E. The aural foreign body space: a review of pediatric ear foreign bodies and a management paradigm. Int J Pediatr Otorhinolaryngol. 2020;132:109871. (Observational; 155 patients) DOI: 10.1016/j.ijporl.2020.109871
30. * American Academy of Family Physicians, American Academy of Otolaryngology-Head and Neck Surgery, American Academy of Pediatrics Subcommittee on Otitis Media With Effusion. Otitis media with effusion. Pediatrics. 2004;113(5):1412-1429. (Clinical practice guidelines) DOI: 10.1542/peds.113.5.1412
31. * Smith ME, Hardman JC, Mehta N, et al. Acute otitis externa: consensus definition, diagnostic criteria and core outcome set development. PLoS One. 2021;16(5):e0251395. (Consensus guidelines) DOI: 10.1371/journal.pone.0251395
40. * Mui S, Rasgon BM, Hilsinger RL Jr, et al. Tympanostomy tubes for otitis media: quality-of-life improvement for children and parents. Ear Nose Throat J. 2005;84(7):418, 420-412, 424. (Retrospective; 379 patients) DOI: 10.1177/014556130508400712
Subscribe to get the full list of 57 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: acute otitis media, AOM, acute otitis externa, AOE, mastoiditis, ear foreign body, ear canal foreign body, myringotomy tubes, tympanostomy tubes, tympanic membrane, perforated tympanic membrane, ear infections, ear pain, pediatric ear, ear canal, otorrhea, ear effusion, caregiver holds, chest-to-chest hold, side-to-chest hold, pneumatic otoscopy
Christina L. Cochran, MD; Kathy W. Monroe, MD
Danielle Federico, MD, FAAP; Kathryn Pade, MD
December 1, 2024
December 1, 2027 CME Information
4 AMA PRA Category 1 Credits™, 4 ACEP Category I Credits, 4 AAP Prescribed Credits, 4 AOA Category 2-B Credits. Specialty CME Credits: Included as part of the 4 credits, this CME activity is eligible for 3 Infectious Disease credits and 1 Pharmacology CME credits, subject to your state and institutional approval.
Pediatric Emergency Medicine Practice • CONTINUE READING
Read this issue today — or unlock the entire library for a little more.
Stay current with a new Pediatric Emergency Medicine Practice issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933