Sir William Osler said: "In the old and debilitated, a knowledge that the onset of pneumonia is insidious and that the symptoms are ill-defined and latent should place the practitioner on his guard and make him very careful."
31 Osler's statement holds true for not only pneumonia but nearly all diseases in the elderly.
"Textbook" symptoms are the exception rather than the rule in the febrile elderly patient. A behavioral change may be the only hint of an underlying infection. At least 75% of all episodes of functional decline in nursing home patients are due to infection.
32 It is a common mistake to assume that the confused 80-year-old is "just demented," when in fact he or she may be a normally intact and independent person with acute delirium secondary to a UTI.
18 Ask family members or caretakers about recent falls, anorexia, decreased activity, new incontinence, or confusion. (See
Table 4.) These may be the only clues to a serious illness. Make an effort to define the patient's baseline functional and mental status. Five minutes on the telephone with the primary care provider or the patient's daughter may prompt life-saving antibiotics instead of an inappropriate prescription for Haldol.

History Of Present IllnessEmergency physicians often hear the familial lament, "Grandpa just hasn't been acting right." This imprecise account can be an important clue to a life-threatening infection. Nearly one-fifth of geriatric patients with a serious infection will present with a vague history and diffuse complaints.
SepsisEmergency physicians correctly predict bacteremia in less than two-thirds of elderly patients.
33 This is often because the associated symptoms in the elderly are so nonspecific. When compared with a younger population, older patients with bacteremia more often present with recurrent falls, malaise, or change in functional or mental status.
34 In one ED study, only a change in mental status and vomiting independently predicted bacteremia in the elderly.
33 These nonspecific symptoms make identifying an infectious source extremely difficult. For example, anorexia, malaise, and nausea are far more common than dysuria or urgency in elderly with urosepsis.
35
PneumoniaSymptoms of pneumonia can also be atypical in the elderly. (See
Table 5; also, see the September 1999 issue of Emergency Medicine Practice, "
Community-Acquired Pneumonia: Deciding Whom To Admit And Which Antibiotics To Use.") Again, Osler wrote, "In senile pneumonia, the temperature may be low and yet brain symptoms are very pronounced."
36 Perhaps the most common symptom of pneumonia in the elderly is a change in mental status, which is seen in up to 65% of cases.
37,38 Ten percent will present with a history of recent falls.
39 To further complicate matters, more than half of elderly patients with pneumonia may lack cough or sputum production; fever is absent in up to 65%.
37,40
Likewise, elderly patients with tuberculosis are less likely to have the classical symptoms of weight loss, night sweats, and hemoptysis.
41Urinary Tract InfectionLower urinary tract symptoms?dysuria, urgency, and frequency?may also be absent in the elderly, particularly in those with indwelling urinary catheters. (See
Table 6.) Symptoms of fever, chills, nausea, and flank and costovertebral pain can be attenuated or even absent.
42 Instead, altered mental status, vomiting, abdominal tenderness, respiratory distress, and rales may dominate the clinical picture.
43 Lack of fever, and even hypothermia, further muddy the diagnostic waters. This atypical presentation may perplex the most astute clinician?in one study of elderly uncatheterized patients with pyelonephritis, the initial diagnosis was incorrect in 21% of cases.
31
 Intra-abdominal Infection
Intra-abdominal Infection
While any type of intra-abdominal infection may occur in the elderly, by far the most common and problematic are appendicitis, cholecystitis, and diverticulitis. The elderly frequently lack the characteristic focal abdominal tenderness, which usually distinguishes these pathologies. (See
Table 7.) Perforation of a viscus and subsequent peritonitis can occur without pain or fever.
44 In fact, confusion and hypotension may be the only symptoms of gastrointestinal infection.
45 This high rate of atypical presentation, and the tendency of the elderly patient to delay presentation, can lead to poor outcome.
46 Although the elderly account for only 5-10% of cases of appendicitis, they account for 60% of the deaths from this disease. Complications such as gangrene, perforation, abscesses, and peritonitis occur in 35-65% of cases, far more often than in younger counterparts.
46 Cholecystitis is the most common cause for surgery in the elderly. In this age group, it is much more likely to progress to gangrene, perforation, suppurative cholangitis, and emphysematous cholecystitis.

Past Medical HistorySome atypical presentations of disease in the elderly are due to underlying illnesses; more than 85% of geriatric patients have one or more chronic diseases.
19 Classical symptoms may be obscured by an exacerbation of these chronic conditions. Pulmonary edema may mask pneumonia, while pre-existing dementia may conceal meningitis. In addition, chronic diseases predispose to specific acute illnesses. (See
Table 8.) For this reason, obtaining a thorough past medical history can be important in the emergency evaluation of the elderly patient. Calls to the medical records department and the primary care provider may be invaluable.

Past medical history can provide important clues to current fever. A history of rheumatic heart disease or a pacemaker places the patient at increased risk for endocarditis.
48-50 Elderly with incontinence are more likely to have infected pressure ulcers or UTIs,
51 while peripheral vascular disease and chronic venous stasis are risk factors for cellulitis.
52 Many elderly are further immunocompromised by diabetes, corticosteroids, malignancy, ESRD, or HIV. Knowledge of these conditions should increase suspicion for a serious infection.
Determine the presence of "hardware" in the elderly patient with fever. An artificial joint, pacemaker, ventriculo-peritoneal shunt, or prosthetic valve may represent a nidus for infection. Dialysis patients are at special risk for infected central lines and shunts.
A thorough medication history is also essential. New medications may cause a "drug fever." More importantly, recent antibiotics may contribute to a partially treated infection or signify a resistant organism. Question the patient or caretaker regarding antipyretic use, which may mask a fever. The elderly are also at risk for chronic salicylate poisoning, which is an occasional cause of hyperpyrexia. Steroids are a red flag. Geriatric patients on steroids may have few or no stigmata of infection. Recent chemotherapy must prompt a CBC to evaluate for neutropenia. Finally, obtain an immunization history, especially for pneumococcal, influenza, and tetanus vaccines.
Physical Exam"In diagnosing infections in the elderly, physicians must learn to expect the unexpected."
19 As emergency physicians, we reflexively associate infection with fever. In the elderly, however, fever is often absent despite serious infection. Thirteen to forty-seven percent of geriatric patients will be afebrile in the presence of a documented infection.
36,39,48,49,52 (See
Table 9.)

Fever is not alone in its diminished association with bacterial pathology. All of the usual suspects?tachycardia, characteristic abdominal pain, and peritoneal signs? are seen less frequently despite serious and often lifethreatening disease. However, what these signs lack in frequency, they gain in significance.
TemperatureIn some cases, fever in the older patient may go unrecognized. A prospective study by Castle et al monitored temperature responses to documented infections in nursing home residents.
54 The standard definition of fever, temperature greater than 101?F, offered only a sensitivity of 40% and a specificity of 99.7% in this population. They demonstrated that lowering the fever criteria to 99?F better predicts infections in the elderly, with a sensitivity of 83% and specificity of 89%.
A significant number of elderly have no fever (defined as 101?F) with documented infection, but they do have a rise of 2.4?F or more from their baseline temperature.55 These studies suggest that a temperature of 99?F or a change in temperature of at least 2?F from baseline in an elderly individual should make the EP suspect a serious underlying infection.7 The presence of hypothermia not only suggests infection, but predicts a poor outcome in the geriatric population.
PulmonaryThe respiratory rate is one of the most valuable aspects of the respiratory exam. Tachypnea (RR > 30 breaths/min) occurs in 26-75% of elderly patients with pneumonia.
39,55 In some cases, a fast respiratory rate may precede other clinical findings of pneumonia by as much as 3-4 days.
56 The fifth vital sign, pulse oximetry, is easily obtained and may illuminate otherwise subtle respiratory compromise. While the presence of crackles on lung auscultation should alert the emergency physician to the possibility of pneumonia, the exam may be misleading due to chronic lung disease or atelectasis.
CardiovascularLike fever, tachycardia can augur serious illness in the elderly. In a cohort of 470 febrile elderly patients presenting to the ED, a heart rate of 120 bpm or greater independently predicted serious illness.
5 In another study, tachycardia was the presenting sign in 15% of elderly patients with pneumonia.
58 However, the absence of tachycardia cannot reassure the emergency physician. Up to 70% of geriatrics with proven bacteremia may lack tachycardia.
34 Seventy-five percent of elderly patients who develop endocarditis have a predisposing valvular or cardiac lesion, and nearly one-third have a prosthetic valve.
47 Although challenging in a noisy ED, the emergency physician should listen carefully for a heart murmur.
AbdominalIf present, abdominal tenderness is an important finding in this population. Right upper-quadrant or epigastric pain is elicited in 74-84% of elderly patients with cholecystitis.
58 Right lower-quadrant pain or tenderness occurs with most cases of appendicitis,
69-72 while left lowerquadrant pain is found in two-thirds of elderly patients with diverticulitis.
63 However, the disturbing corollary is that a significant number of elderly patients who present with a surgical emergency have no significant abdominal tenderness?estimated at up to 25% in cholecystitis, 34% in appendicitis, and 13-30% in diverticulitis.
46,63,64NeurologicalEstablishing orientation and general mental function in the elderly is essential. As mentioned before, a new decline in mental status may be the only objective sign of a life-threatening illness. The emergency physician should search for focal neurological findings. A surprising 40% of elderly with bacterial meningitis have a focal neurological deficit, while nearly half lack meningismus on presentation.
65-68 (See
Table 10.) The finding of a "stiff neck" may be misleading, as the nuchal rigidity associated with meningitis can be difficult to distinguish from chronic cervical arthritis or chronic neurologic disease
such as Parkinsonism.
 Genitourinary
GenitourinaryCostovertebral angle tenderness may represent an upper urinary tract infection, though some studies suggest that this finding occurs in less than half of the elderly with pyelonephritis.
69 Suprapubic tenderness may indicate cystitis. A rectal examination is necessary to detect prostatitis in the elderly male. However, prostatic massage is not indicated to obtain cultures, as this practice induces bacteremia. On occasion, an examination of the external genitalia may reveal redness, tenderness, or discharge. Any vaginal or penile discharge should be cultured?remember that even octogenarians contract sexually transmitted diseases.
Skin/Soft TissueBegin the skin examination by completely undressing the geriatric patient. Cellulitis can be easily overlooked if the lighting is poor or the patient is only partially disrobed. Look for surgical scars, which may reveal a wound infection or clues to the patient's medical history, such as prior splenectomy, pacemaker insertion, or artificial joint. While the patient may demonstrate peripheral evidence of endocarditis, petechiae, Osler nodes, and Janeway lesions are all less common in the elderly.
49Make a special effort to find pressure ulcers in the immobile, incontinent, or nursing home patient. Twenty to twenty-five percent of nursing home inhabitants have skin ulcers, and 10-65% of these will be infected.
70,71 The most common locations include the heels, the sacrum, ischial tuberosities, and the buttocks? all areas that can easily be overlooked on a superficial exam of a supine patient.
71 Infected ulcers are suggested by expanding erythema, purulent drainage, foul odor, or necrotic tissue.
50 Chronic non-healing ulcers may indicate an underlying osteomyelitis, especially when bone is exposed.
Finally, inspect the joints in geriatric patients, especially those with prosthesis. Joints with erythema, warmth, or effusion may be infected and should be aspirated for synovial fluid analysis. Pain on range of motion is the most reliable sign of a septic joint.
Diagnostic StudiesSome argue that the workup of fever at the extremes of age is simple?just do everything. While this hyperbole represents an oversimplification, it holds a kernel of truth.
Although the history and physical examination should guide test selection, the emergency physician should use laboratory and imaging studies liberally in the febrile senior, despite the current climate of cost-reduction.
If an infectious cause for fever is suspected, helpful tests may include a complete blood count and differential, at least two sets of blood cultures, urinalysis with culture, chest x-ray, and a creatinine level. The Clinical Pathway "Treatment Of The Elderly Patient With Pneumonia" outlines a general approach to the diagnostic and initial management dilemmas in the febrile elderly.
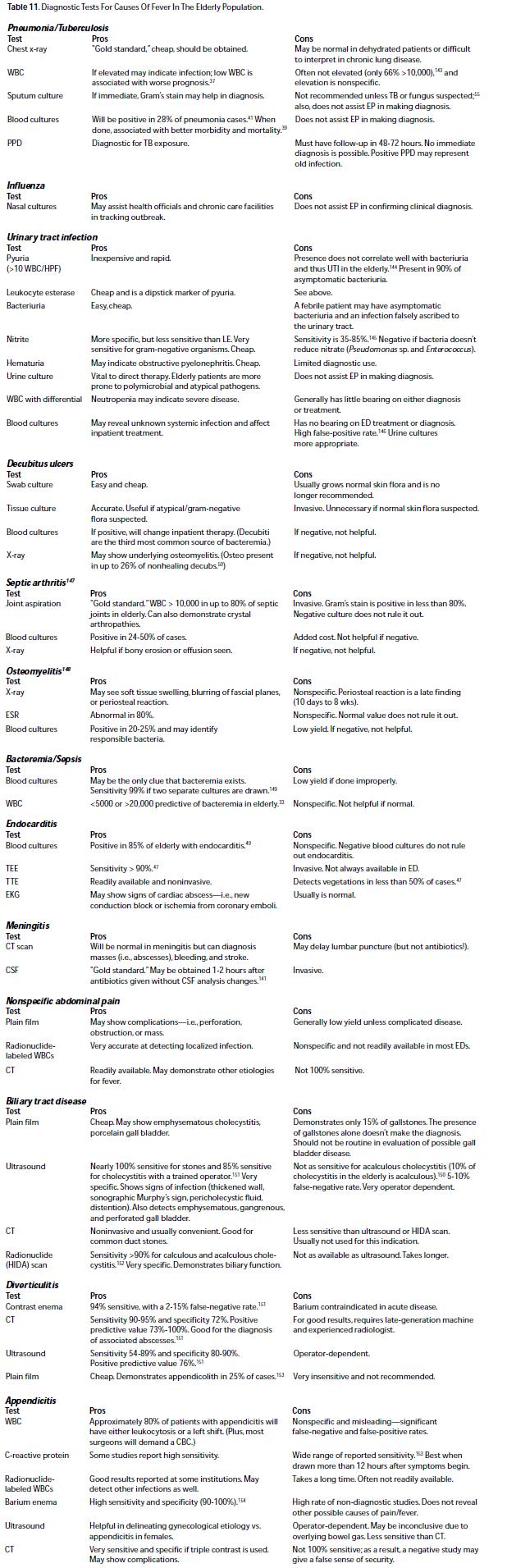
Table 11 lists the pros and cons of specific laboratory and imaging tests for the most common infections in this population.
 Pulmonary Infections
Pulmonary InfectionsFew diagnostic tests can challenge the chest x-ray in terms of "bang for the buck"?it is money well spent in the evaluation of the febrile older adult. One large prospective study of patients older than 75 with chest complaints or fever demonstrated a greater than 80% incidence of acute findings on chest X-ray.
72 Other studies demonstrate that almost one-quarter of elderly patients presenting with acute confusion and a benign physical exam will have pneumonia by x-ray.
38 When possible, always obtain PA and lateral chest views. Decubitus views of the chest may be indicated if an effusion is noted or suspected.
In some patients, however, the chest film may be misleading. The acutely ill and dehydrated patient may lack a characteristic infiltrate despite pneumonia. In case of strong suspicion, a repeat x-ray after adequate rehydration may demonstrate an infiltrate. On the other hand, many chronic diseases that predispose to bacterial pneumonia, such as COPD and CHF, may obscure radiographic findings.
Once the chest radiograph demonstrates pneumonia, additional tests may be helpful. Pleural fluid in the setting of a fever should be aspirated and sent for Gram's stain, culture, cell count, LDH, pH, glucose, protein, and cytology. In general, sputum cultures are not useful in the initial evaluation of pneumonia,
38 unless tuberculosis or fungi are likely. However, blood cultures will be positive in up to 28% of pneumonia cases and may help guide inpatient therapy.
36,39 Consider PPD, fungal, and anergy panels when clinically indicated. While nasal cultures can be obtained if influenza virus is considered, these do not assist the emergency physician in the clinical diagnosis. Finally, an arterial blood gas can quantify hypoxemia or hypercarbia and may help determine the disposition. However, pulse oximetry is adequate to evaluate most patients with pneumonia who have no history of COPD.
Urinary Tract InfectionThe diagnosis of UTI in the elderly patient can be difficult for several reasons. First, the elderly are prone to asymptomatic bacteriuria. Up to 34% of elderly women have asymptomatic bacteriuria at any one time. Some authorities believe that the majority of elderly women and many older men have at least one episode of asymptomatic bacteriuria during their lifetimes.
73 Thus, an elderly patient presenting with bacteriuria and a fever presents a diagnostic dilemma: Is this a UTI or rather the presentation of pneumonia in a patient with coincident asymptomatic bacteriuria? For this reason, it is prudent to explore all potential sources for a fever before attributing it to the urinary tract.
Even the quantitative urine culture is not completely reliable. Definitive diagnosis of UTI has traditionally been defined as greater than 10
5 uropathogens/mL. This relatively arbitrary number was derived over 20 years ago based on studies of young women and does not uniformly apply to the elderly. Nearly one-third of patients with proven UTI have a bacterial count of less than 10
5 cfu/mL.
74,75 Some authorities propose that for symptomatic women or for patients with indwelling catheters, growth of 102 cfu/mL of a single bacterial pathogen is sufficient to diagnose UTI. For men, 10
5 cfu/ mL is still the accepted standard, though some suggest it be lowered to 10
4 cfu/mL or even 10
3 cfu/mL.
73,78Other traditional markers of UTI, such as pyuria, leukocyte esterase, and nitrite, are also less reliable in the elderly patient. Pyuria is a poor predictor of bacteriuria; white cells are present in the urine of only 36-79% of elderly patients with UTIs.
74,79The method of obtaining urine for analysis is often as important as the specimen itself. Catheter specimens are preferred over midstream clean catch specimens in women. False-positive rates as high as 57% have been documented in elderly women when midstream specimens are compared with suprapubic aspiration.
79 Patients who present with an indwelling catheter should have the catheter changed before obtaining a urine sample. One study shows as many as one-quarter of specimens obtained from a chronic indwelling catheter misrepresent the true urine pathogens.
80Keeping these caveats in mind, the emergency physician should not hesitate to perform a urinalysis on any febrile senior. For elderly females with isolated lower tract symptoms and no comorbid conditions, a urinalysis alone will suffice. Obtain a creatinine level for females with any evidence of upper-tract disease. Obtain blood cultures in addition to urine cultures in patients with complicated infections. This would include those with indwelling Foley catheters, recent antibiotic treatment, or concurrent stone or stent. In men with any upper- or lower-tract symptoms, suspect urinary retention secondary to prostatic enlargement. Determine post-void residual by catheterization or by bladder sonogram.
Radiographic imaging of the urinary system is necessary in the ED if the emergency physician suspects
the patient has an infected ureteral stone or stent, or in the case of suspected intrarenal or perinephric abscess. Consider perinephric abscess in patients with persistent fever and bacteriuria despite appropriate treatment; it is particularly likely in diabetics. Other renal imaging is generally deferred to the consultant. The goal of imaging studies is to identify any surgically correctable abnormalities of the urinary tract?urinary tract obstruction or intrarenal or perinephric abscess. Renal ultrasound reliably detects hydronephrosis associated with obstruction, while an abdominal CT with intravenous contrast best defines an intrarenal or perinephric abscess.
Indwelling CathetersThe emergency physician should strongly suspect a urinary source in any febrile elderly patient with an indwelling catheter, as two-thirds of these febrile episodes are caused by UTI.
81 The use of indwelling catheters is the single most important risk factor for the development of urinary tract infections in the institutionalized elderly.
82 Despite this fact, their use is ubiquitous; at any given time, more than 100,000 patients in U.S. nursing homes have an indwelling urethral catheter.
83 Catheterized patients develop bacteriuria at a rate of 3-10% per day, making bacteriuria a nearly universal finding in patients catheterized for longer than one month.
84 As a result, it is important to search for other causes of fever in this population before automatically attributing it to a UTI. On the other hand, chronic bacteriuria can lead to fever, UTI, pyelonephritis, and urosepsis. It is estimated that 2-4% of patients with bacteriuria develop bacteremia. Other febrile complications associated with long-term catheterization include chronic pyelonephritis, urethritis, epididymitis, scrotal abscess, prostatitis, and prostatic abscess.
85
Abdominal InfectionsFor the febrile elderly patient with abdominal findings, a CBC with differential, liver function tests, amylase, and lipase may be helpful. Given the incidence of atypical presentations and increased morbidity and mortality in the elderly, the emergency physician should maintain a low threshold for radiological imaging. Obtain a right upper quadrant ultrasound if cholecystitis is considered. The diagnosis of diverticulitis is generally made clinically, though complications such as obstruction and abscesses are best seen on CT. Radiocontrast enema may actually exacerbate acute diverticular disease, and physicians should employ a water-based contrast medium if the process is used at all. Helical CT using triple contrast (oral, rectal, and intravenous) is becoming an important diagnostic tool in the evaluation of appendicitis, demonstrating accuracy rates of 98%.
86







 678-366-7933
678-366-7933