Table of Contents
About This Issue
Renal and genitourinary (GU) injury can be a hidden source of morbidity and mortality for patients who experience trauma from blunt or penetrating forces. A thorough history as well as strategic laboratory testing and imaging can improve a patient’s chances for recovery without serious sequelae. In this issue, you will learn:
How the type of injury (blunt vs penetrating) and the mechanism (falls, sports-related trauma, sexual activity, blows, gunshot/stabbing, etc) can be clues to revealing the injured organs.
The best practices for the polytrauma patient with serious injuries: how to tell which GU injuries are emergent, urgent, or less serious.
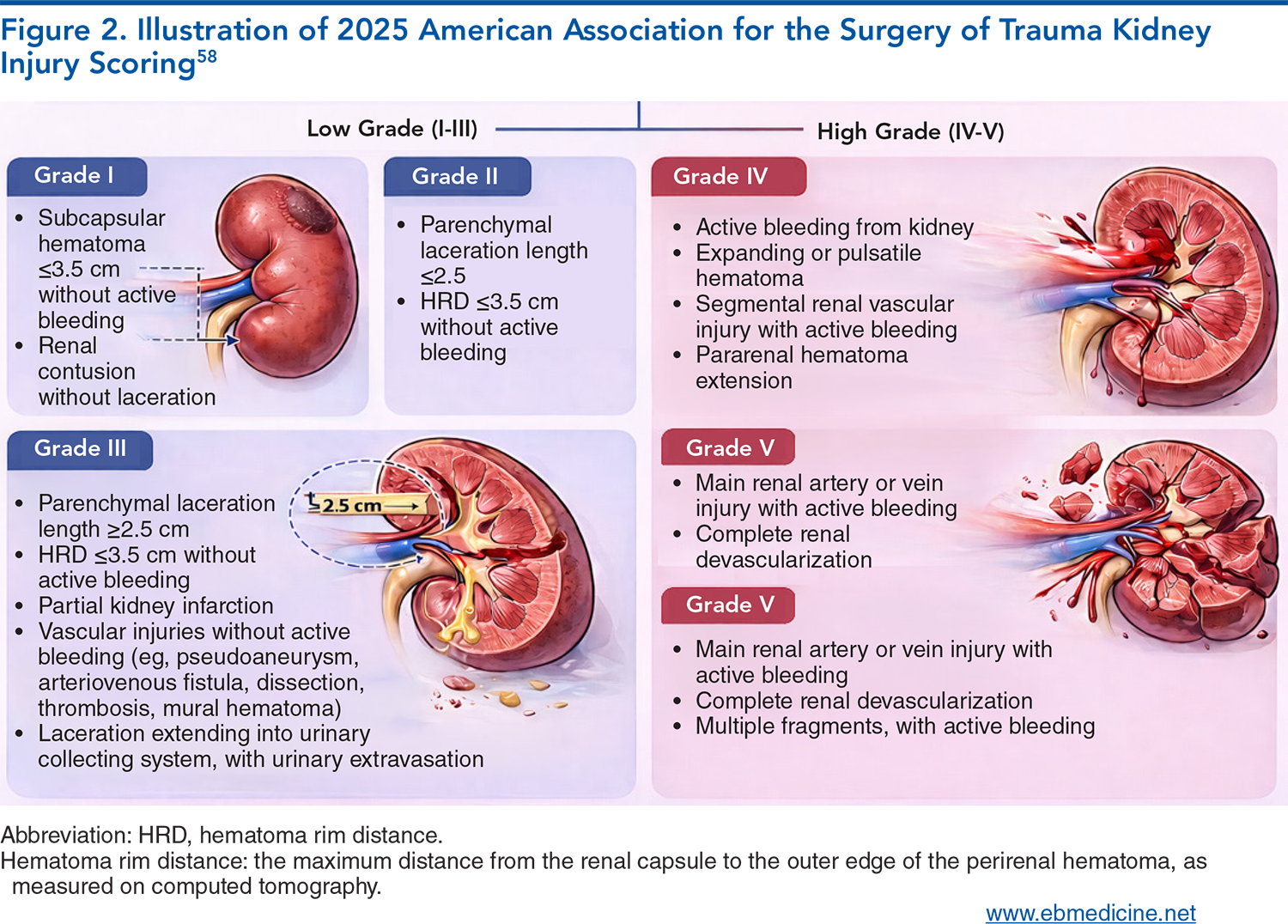
Kidney injury grading, I to V: what the 2025 changes to the AAST kidney injury scoring system include.
Which injuries warrant immediate surgical intervention, which injuries can wait, and when consult and transfer are needed.
What hematuria – or the lack of it – indicates about where a GU injury is.
How and when a urinary catheter should be placed, and when a suprapubic catheter is safer.
CT, CT cystography, retrograde urethrogram, ultrasound, or MRI: when each imaging modality is indicated.
- About This Issue
- Abstract
- Case Presentations
- Introduction
- Critical Appraisal of the Literature
- Epidemiology
- Etiology and Pathophysiology
- Kidneys and Ureters
- Bladder
- Male Genitalia
- Female Genitalia
- Differential Diagnosis
- Prehospital Care
- Emergency Department Evaluation
- History
- Ability to Void, Dysuria, and Hematuria
- Physical Examination
- Diagnostic Studies
- Laboratory Studies
- Baseline Renal Function
- Urinalysis
- Hematuria in Blunt Trauma
- Hematuria in Penetrating Trauma
- Imaging
- Computed Tomographic Imaging
- Computed Tomographic Cystography
- Computed Tomographic Angiography
- Retrograde Urethrogram
- Ultrasound
- Magnetic Resonance Imaging
- Treatment
- Catheters and Urinary Diversion
- Suprapubic Catheterization
- Alternative Methods of Urinary Diversion
- Surgery
- Interventional Radiology
- Admission
- Special Populations
- Pediatric Patients
- Older Patients
- Controversies and Cutting Edge
- Magnetic Resonance Imaging
- Nonoperative Management
- Contrast-Enhanced Ultrasound
- Disposition
- Transfer
- Consultation
- Urinary Catheter Care
- Time- and Cost-Effective Strategies
- Risk Management Pitfalls for Emergency Department Management of Patients With Renal and Genitourinary Trauma
- Summary
- 5 Things That Will Change Your Practice
- Case Conclusions
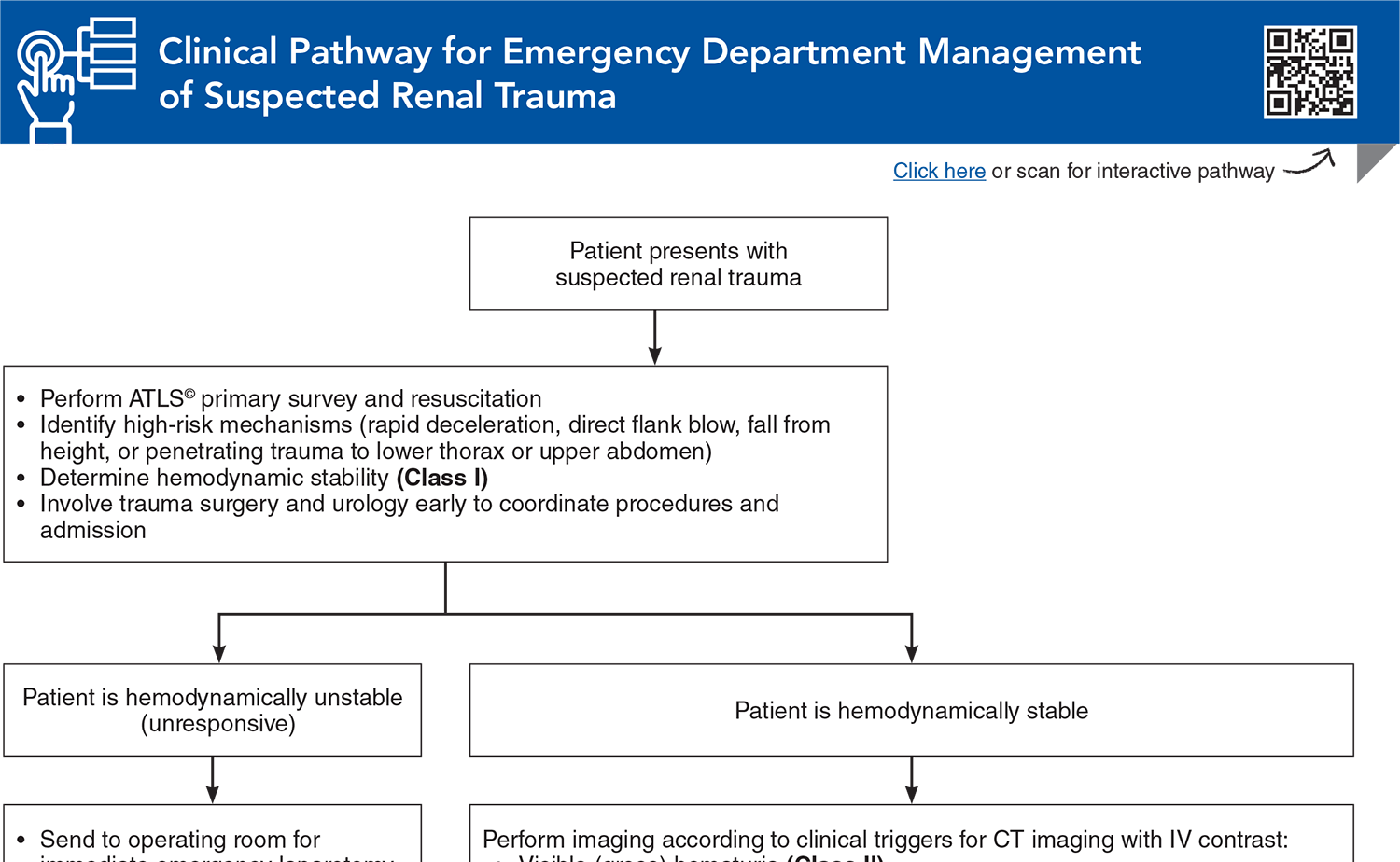
- Clinical Pathway for Emergency Department Management of Suspected Renal Trauma
- Tables and Figures
- References
Abstract
For polytrauma patients who may have life-threatening injuries, renal and genitourinary trauma may be overlooked initially, but a delayed or missed diagnosis of these injuries may result in potentially preventable complications. This review provides a best-practice approach to the diagnosis and management of renal and genitourinary injuries, with an emphasis on the systematic approach needed to identify subtle injuries and avoid long-term sequelae such as hypertension, incontinence, urethral stricture, erectile dysfunction, chronic kidney disease, and nephrectomy.
Case Presentations
- He appears to be intoxicated and was involved in an altercation. He has bruises and red marks that look like shoe prints over his abdomen, flanks, and chest.
- On his right flank, he has a 1- by 2-cm wound he said was made by a screwdriver.
- His temperature is 36.5°C; heart rate, 135 beats/min; blood pressure, 85/49 mm Hg; respiratory rate, 24 breaths/min; and oxygen saturation, 97%.
- You consider whether a urinalysis will help in working up this patient. What kind of special imaging is he going to need?
- She appears to be intoxicated, and EMS tells you that she was the unrestrained and ejected passenger in a high-speed, rollover, single-car crash.
- Her temperature is 38.3°C; heart rate, 107 beats/min; blood pressure, 86/68 mm Hg; respiratory rate, 18 breaths/min; and oxygen saturation, 94%.
- EMS has placed a pelvic binder, and a tense, swollen abdomen extends above it.
- During the resuscitation, you notice she is bleeding briskly from her vagina.
- Should you place a Foley catheter? Do you need to page urology and trauma as well?
- He is screaming in pain and has an obvious chest wall deformity, with crepitus.
- He has a massive hematoma to his perineum and scrotum, a testicle that appears dislocated and free from the scrotum, and a deformity to his penile shaft. There is gross blood at the urethral meatus.
- His temperature is 36.1°C; heart rate, 144 beats/min; blood pressure, 103/81 mm Hg; respiratory rate, 31 breaths/min; and oxygen saturation, 88%.
- How do you begin assessing this patient’s genitourinary trauma? Should you place a suprapubic catheter?
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
Clinical Pathway for Managing Patients Presenting with Acute Diarrhea in Urgent Care
Subscribe to access the complete Clinical Pathway to guide your clinical decision making.
Tables and Figures
Subscribe for full access to all Tables and Figures.
Buy this issue and
CME test to get 4 CME credits.
Key References
Following are the most informative references cited in this paper, as determined by the authors.
26. * Serafetinidis E, Campos-Juanatey F, Hallscheidt P, et al. Summary paper of the updated 2023 European Association of Urology guidelines on urological trauma. Eur Urol Focus. 2024;10(3):475-485. (Review) DOI: 10.1016/j.euf.2023.08.011
33. * Matta R, Keihani S, Hebert KJ, et al. Proposed revision of the American Association for Surgery of Trauma Renal Organ Injury Scale: secondary analysis of the Multi-institutional Genitourinary Trauma Study. J Trauma Acute Care Surg. 2024;97(2):205-212. (Secondary analysis of a multicenter retrospective study; 549 patients)
45. * Aziz HA, Bugaev N, Baltazar G, et al. Management of adult renal trauma: a practice management guideline from the Eastern Association for the Surgery of Trauma. BMC Surg. 2023;23(1):22. (Practice guidelines) DOI: 10.1186/s12893-023-01914-x
62. * Kitrey ND, Campos-Juanatey F, Hallscheidt P, et al. EAU guidelines on urological trauma. Accessed March 15, 2026. (Practice guidelines)
99. * Reddy D, Laher AE, Moeng M, et al. Bladder trauma: a guideline of the guidelines. BJU Int. 2024;133(4):365-374. (Review) DOI: 10.1111/bju.16236
104. * Patel AB, Osterberg EC, Satarasinghe PN, et al. Urethral injuries: diagnostic and management strategies for critical care and trauma clinicians. J Clin Med. 2023;12(4). (Review) DOI: 10.3390/jcm12041495
Subscribe to get the full list of 138 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: kidney, ureter, bladder, urethra, genital, pelvis, penis, scrotum, flank, catheter, blunt, penetrating









 678-366-7933
678-366-7933
