

|
|
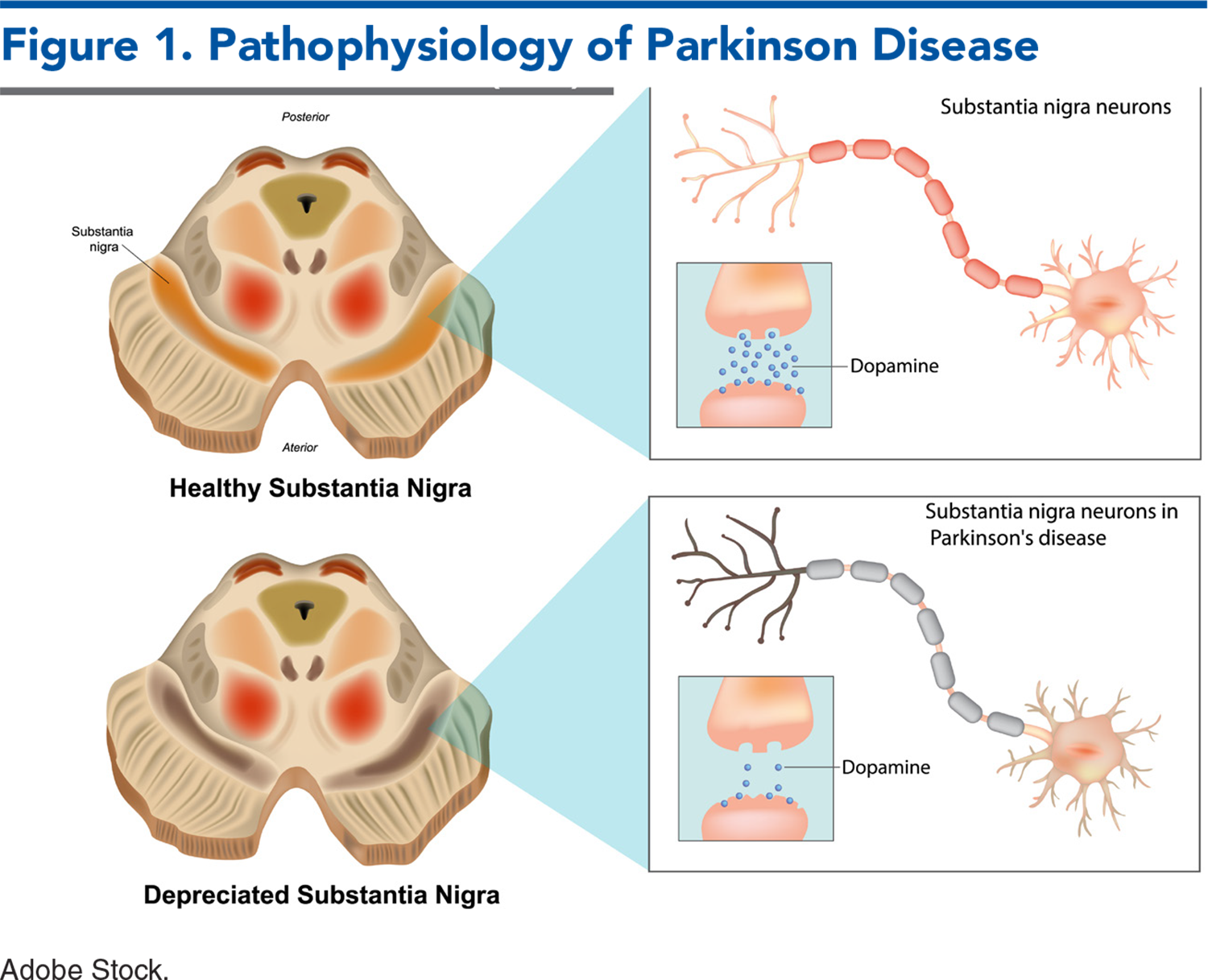
This issue reviews 3 neurological conditions that can cause or complicate a patient‘s emergency department presentation: Parkinson disease, myasthenia gravis, and multiple sclerosis. Parkinson disease is a common comorbidity, and can be exacerbated in the ED if not managed expeditiously. Myasthenia gravis carries the potential for significant respiratory compromise and requires swift recognition and emergency care. Multiple sclerosis has many manifestions, stages, and treatments that emergency clinicians need to understand to best manage flares. This review presents a summary of the presentations, the common pitfalls, and the roles of various therapeutics in managing patients with chronic neurologic disease.
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
![]()
![]() 1. “That Parkinson patient had a feeding tube that fell out. I thought it could be replaced in the morning.” The tube may not be a feeding tube; it may be used for a continuous enteral carbidopa/levodopa administration. Without it, the patient may not be receiving their medication, and it needs to be replaced immediately.
1. “That Parkinson patient had a feeding tube that fell out. I thought it could be replaced in the morning.” The tube may not be a feeding tube; it may be used for a continuous enteral carbidopa/levodopa administration. Without it, the patient may not be receiving their medication, and it needs to be replaced immediately.
4. “The oxygen saturation for my myasthenia gravis patient was fine!” Myasthenia gravis is fundamentally a problem of ventilation rather than oxygenation. The first metabolic sign is hypercarbic respiratory acidosis, although even this may be compensated. A normal oxygen saturation does not indicate normal ventilation but rather, normal oxygenation.
9. “It's OK if the MS patient‘s baclofen pump stopped. We can give baclofen orally.” Oral baclofen doses do not achieve the same effects as IV or intrathecal dosing. Abrupt withdrawal is a true emergency and must be managed aggressively with high doses of IV GABA-ergic medications such as benzodiazepines and/or propofol. MRI may reset the pump settings, causing an abrupt, occult drop in dosage.
Subscribe for full access to all Tables and Figures.
Buy this issue and
Following are the most informative references cited in this paper, as determined by the authors.
11. * Cheron J, Deviere J, Supiot F, et al. The use of enteral access for continuous delivery of levodopa-carbidopa in patients with advanced Parkinson’s disease. United European Gastroenterol J. 2017;5(1):60-68. (Retrospective cohort; 27 patients) DOI: 10.1177/2050640616650804
12. * Sharma VD, Patel M, Miocinovic S. Surgical treatment of Parkinson’s disease: devices and lesion approaches. Neurotherapeutics. 2020;17(4):1525-1538. (Review) DOI: 10.1007/s13311-020-00939-x
13. * Dresser L, Wlodarski R, Rezania K, et al. Myasthenia gravis: epidemiology, pathophysiology and clinical manifestations. J Clin Med. 2021;10(11):2235. (Review) DOI: 10.3390/jcm10112235
15. * Gummi RR, Kukulka NA, Deroche CB, et al. Factors associated with acute exacerbations of myasthenia gravis. Muscle Nerve. 2019;60(6):693-699. (Retrospective chart review; 127 patients) DOI: 10.1002/mus.26689
21. * Sanders DB, Wolfe GI, Benatar M, et al. International consensus guidance for management of myasthenia gravis: executive summary. Neurology. 2016;87(4):419-425. (Consensus guidance) DOI: 10.1212/WNL.0000000000002790
25. * Elsheikh B, Arnold WD, Gharibshahi S, et al. Correlation of single-breath count test and neck flexor muscle strength with spirometry in myasthenia gravis. Muscle Nerve. 2016;53(1):134-136. (Prospective single blind study; 31 patients) DOI: 10.1002/mus.24929
38. * Kraker JA, Xu SC, Flanagan EP, et al. Ocular manifestations of multiple sclerosis: a population-based study. J Neuroophthalmol. 2024;44(2):157-161. (Population-based retrospective cohort study; 200 patients) DOI: 10.1097/WNO.0000000000002116
40. * Pelletier J, Sugar D, Koyfman A, et al. Multiple sclerosis: an emergency medicine-focused narrative review. J Emerg Med. 2024;66(4):e441-e456. (Narrative review) DOI: 10.1016/j.jemermed.2023.12.003
46. * Aletreby W, Alharthy A, Brindley PG, et al. Optic nerve sheath diameter ultrasound for raised intracranial pressure: a literature review and meta-analysis of its diagnostic accuracy. J Ultrasound Med. 2022;41(3):585-595. (Systematic review and meta-analysis; 18 studies) DOI: 10.1002/jum.15732
49. * Pakpoor J, Saylor D, Izbudak I, et al. Emergency department MRI scanning of patients with multiple sclerosis: worthwhile or wasteful? AJNR Am J Neuroradiol. 2017;38(1):12-17. (Retrospective cohort study; 142 patients) DOI: 10.3174/ajnr.A4953
Subscribe to get the full list of 78 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: Parkinson, myasthenia gravis, multiple sclerosis, tremor, dyskinesia, rigidity, carbidopa, levodopa, respiratory, beta blocker, neuromuscular, negative inspiratory force, BPAP, diplopia, pseudoflare, relapse, optic, Lhermitte, McDonald, MRI, lumbar puncture, corticosteroids, baclofen
Jeremy Rose, MD, MPH, FRCPC, FACEP; Caroline W. Burmon, MD; John Rozehnal, MD
Jay Bernstein, MD, MPH, MS, FACEP; Linda Papa, MD, CM, MSc, CCFP, FRCP(C), FACEP; Benjamin Schnapp, MD, MEd
May 1, 2025
May 1, 2028 CME Information
4 AMA PRA Category 1 Credits™, 4 ACEP Category I Credits, 4 AAFP Prescribed Credits, 4 AOA Category 2-B Credits. Specialty CME Credits:Included as part of the 4 credits, this CME activity is eligible for 2 Pharmacology CME credits, subject to your state and institutional approval.
Accredited By





Our Partners


 678-366-7933
678-366-7933

