Table of Contents
About This Issue
Medical advancements have enabled many children to live longer with the support of complex medical technologies. By understanding technology-specific complications and emphasizing collaborative care, emergency clinicians can deliver safer, more effective treatment for this high-risk pediatric population. This issue provides an evidence-based approach for emergency management of children with medical complexity who use 3 commonly encountered technologies: tracheostomies, enteral feeding tubes, and cerebrospinal fluid shunts. In this issue, you will learn:
Conditions that should be on the differential diagnosis for patients with possible complications from tracheostomies, feeding tubes, and cerebrospinal fluid shunts
Recommendations for prehospital care for patients with these medical technologies, with an overall focus on stabilization, prevention of complications, and timely transfer to definitive care
The value of speaking to both caregivers and the patient, to the extent they are able to communicate, when taking the history
The importance of understanding the child’s baseline levels and normal vital sign ranges
Recommendations for diagnostic studies, including when laboratory studies or imaging studies are indicated
Guidance for management of common complications of tracheostomies, feeding tubes, and cerebrospinal fluid shunts
Recommendations for disposition planning for children with these medical complexities
- About This Issue
- Abstract
- Case Presentations
- Introduction
- Critical Appraisal of the Literature
- Etiology and Pathophysiology
- Tracheostomy
- Feeding Tube
- Cerebrospinal Fluid Shunt
- Differential Diagnosis
- Tracheostomy
- Feeding Tube
- Cerebrospinal Fluid Shunt
- Prehospital Care
- Tracheostomy
- Feeding Tube
- Cerebrospinal Fluid Shunt
- Emergency Department Evaluation
- History
- Tracheostomy
- Feeding Tube
- Cerebrospinal Fluid Shunt
- Physical Examination
- Tracheostomy
- Feeding Tube
- Cerebrospinal Fluid Shunt
- Diagnostic Studies
- Tracheostomy
- Feeding Tube
- Cerebrospinal Fluid Shunt
- Treatment
- Tracheostomy
- Obstruction or Dislodgement
- Bleeding
- Infection and Granulation
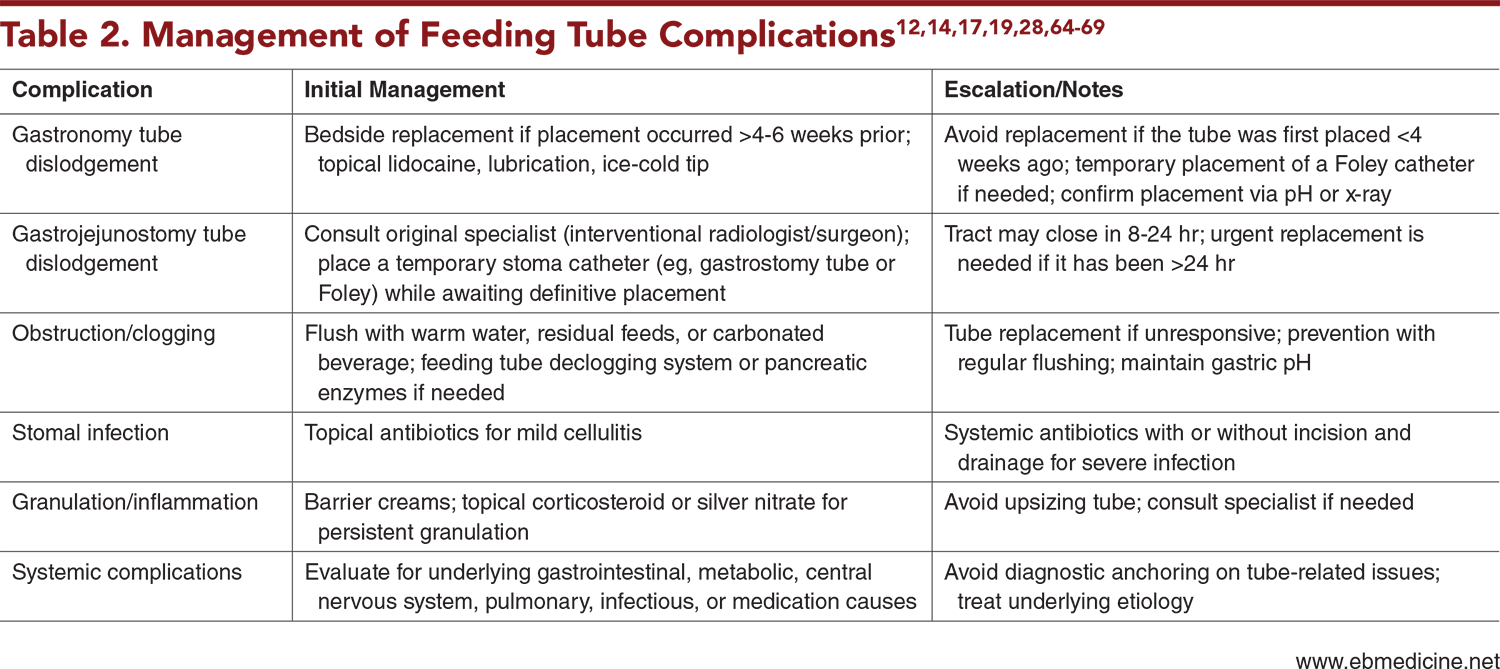
- Feeding Tube
- Dislodgement
- Obstruction
- Leakage and Malposition
- Granulation and Infection
- Cerebrospinal Fluid Shunt
- Obstruction and Breakage
- Shunt Reprogramming
- Infection
- Cerebrospinal Fluid Pseudocyst
- Special Circumstances
- Controversies and Cutting Edge
- Disposition
- Tracheostomy
- Feeding Tube
- Cerebrospinal Fluid Shunt
- 5 Things That Will Change Your Practice
- Risk Management Pitfalls for Emergency Department Management of Children With Tracheostomies, Feeding Tubes, and Cerebrospinal Fluid Shunts
- Summary
- Time- and Cost-Effective Strategies
- Case Conclusions
- Clinical Pathways
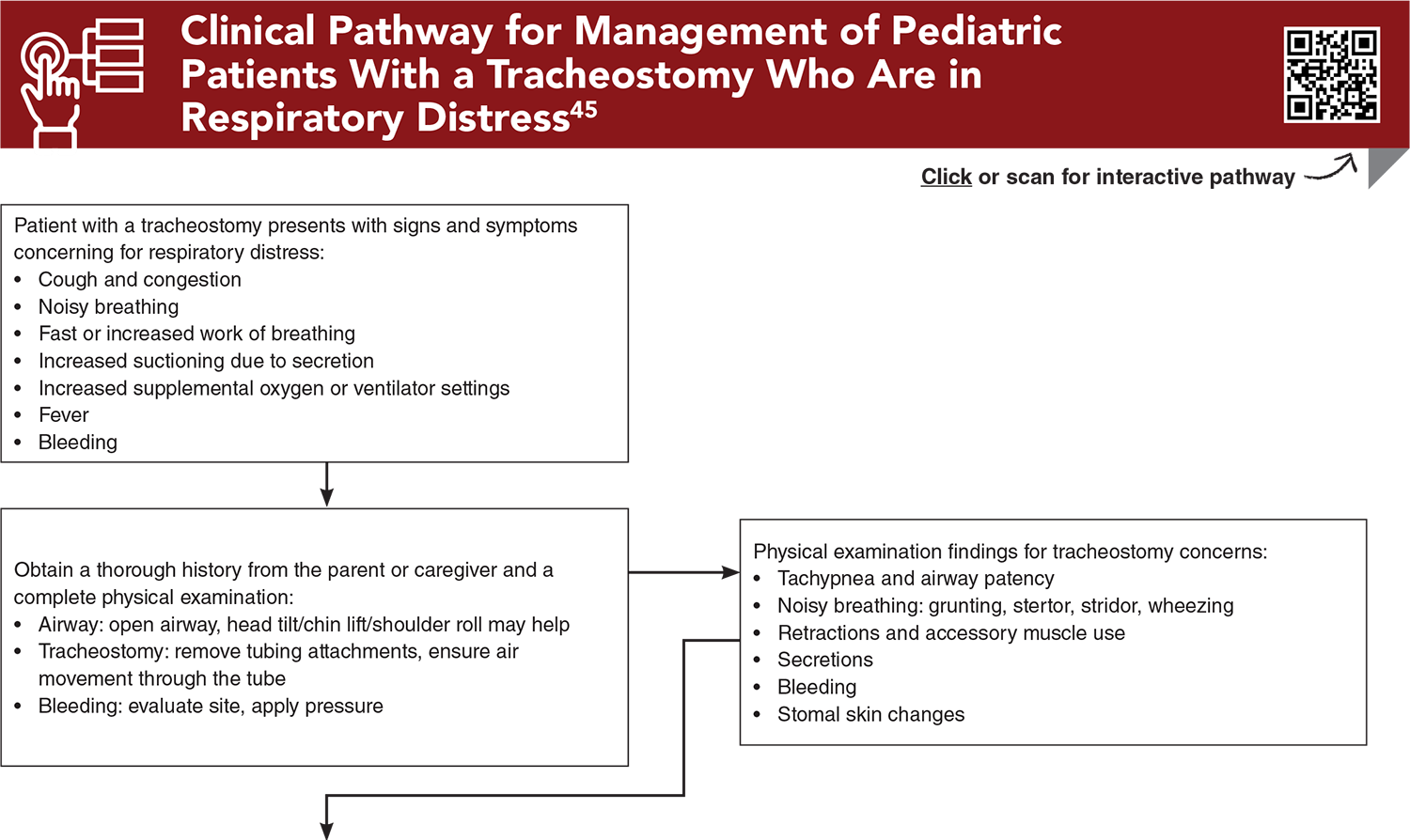
- Clinical Pathway for Management of Pediatric Patients With a Tracheostomy Who Are in Respiratory Distress
- Clinical Pathway for Management of Feeding Tube Dislodgement in Pediatric Patients
- Clinical Pathway for Management of Pediatric Patients With Cerebrospinal Fluid Shunt Malfunction
- Tables and Figures
- References
Abstract
Children with medical complexity represent a growing population in emergency medicine, and many of these children depend on medical technology. This issue provides an evidence-based framework for the emergency management of children with 3 commonly encountered technologies: tracheostomies, enteral feeding tubes, and cerebrospinal fluid shunts. Distinct risks, including obstruction, dislodgement, infection, and mechanical failure, are discussed. Strategies for early recognition, stabilization, and incorporation of caregiver input are reviewed to improve outcomes and reduce medical errors. By understanding technology-specific complications and emphasizing collaborative care, emergency clinicians can deliver safer, more effective treatment for this high-risk pediatric population.
Case Presentations
- The boy was born at 27 weeks’ gestation. He has cerebral palsy and developmental delay. He is dependent on a gastrostomy tube, tracheostomy, and a home ventilator. His parents called EMS with concern for respiratory distress and increased oxygen requirement on his ventilator. They first noticed a minor increase in his tracheostomy secretions a few days prior to presentation, but he was otherwise at his baseline until he became febrile yesterday afternoon. Today, the patient continues to have fever of 38°C, and his parents noticed increased and thicker tracheostomy secretions, an increase in his baseline retractions, and desaturations requiring increased oxygen on his ventilator.
- The boy’s vital sign are: temperature, 38.2°C; heart rate, 135 beats/min; blood pressure, 85/40 mm Hg; respiratory rate, 32 breaths/min; and oxygen saturation, 95%. His tracheostomy tube is in place, with thick yellow secretions. He has intercostal retractions and a soft abdomen.
- A 16-month-old girl with a history of autism, epilepsy, and gastrostomy tube dependence presents with vomiting and intolerance of gastrostomy tube feeds...
- The girl’s mother reports that symptoms started 2 days ago with 1 to 2 episodes of nonbloody, nonbilious emesis per day. Today, she was unable to tolerate any of her gastrostomy tube feeds, so her mother brought her in. The mother tells you that the emesis has remained nonbloody and nonbilious. The girl has had 3 wet diapers so far today, and her last bowel movement was yesterday and was normal.
- The patient’s vital signs are unremarkable. On examination, her abdomen is soft. Her gastrostomy tube site is clean, dry, and intact. Her capillary refill time is 2 to 3 seconds. A point-of-care glucose reading is 82 mg/dL.
- What is the differential diagnosis for this presentation?
- The patient woke up this morning with a headache that has progressively worsened in severity, and this afternoon he had 2 episodes of nonbloody, nonbilious emesis. Upon arrival, the parents noted he was difficult to arouse.
- On examination, the boy’s vital signs are: temperature, 37°C; heart rate, 95 beats/min; blood pressure, 85/44 mm Hg; respiratory rate, 22 breaths/min; and oxygen saturation, 98%. He has a Glasgow Coma Scale score of 10. He opens his eyes and localizes to pain. His pupils are equal, round, and reactive to light. During the examination, he is not speaking with appropriate words.
- What imaging modality would be most helpful in establishing a diagnosis for this patient?
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
Clinical Pathway for Management of Pediatric Patients With a Tracheostomy Who Are in Respiratory Distress
Subscribe to access the complete Clinical Pathway to guide your clinical decision making.
Tables and Figures
Subscribe for full access to all Tables and Figures.
Buy this issue and
CME test to get 4 CME credits.
Key References
Following are the most informative references cited in this paper, as determined by the authors.
1. * Kuo DZ, Houtrow AJ, Council on Children With Disabilities. Recognition and management of medical complexity. Pediatrics. 2016;138(6):e20163021. (Clinical report) DOI: 10.1542/peds.2016-3021
7. * Pulcini CD, Dubuque A, Lamberson M, et al. Pediatric emergency medicine physicians’ perspectives on emergency care of children with medical complexity: a multi-institution mixed-methods assessment. Pediatr Emerg Care. 2022;38(8):e1423-e1427. (Survey; 151/495 respondents) DOI: 10.1097/PEC.0000000000002712
12. * Szydlowski EG, Cronan KM, Fein JA, et al. Technology-assisted children. In: Shaw KN, Bachur RG, Chamberlain JM, et al, eds. Fleisher & Ludwig’s Textbook of Pediatric Emergency Medicine. 8th ed: Wolters Kluwer; 2021. (Textbook chapter)
14. * Natesan A, Behar S. Technology-dependent children. Emerg Med Clin North Am. 2021;39(3):641-660. (Review) DOI: 10.1016/j.emc.2021.04.014
22. * Hanak BW, Bonow RH, Harris CA, et al. Cerebrospinal fluid shunting complications in children. Pediatr Neurosur. 2017;52(6):381-400. (Review) DOI: 10.1159/000452840
45. * Doherty C, Neal R, English C, et al. Multidisciplinary guidelines for the management of paediatric tracheostomy emergencies. Anaesthesia. 2018;73(11):1400-1417. (Practice guideline) DOI: 10.1111/anae.14307
48. * Bober J, Rochlin J, Marneni S. Ventriculoperitoneal shunt complications in children: an evidence-based approach to emergency department management. Pediatr Emerg Med Pract. 2016;13(2):1-22. (Review)
64. * Shah R, Shah M, Aleem A. Gastrostomy tube replacement. In: StatPearls. NCBI Bookshelf version. StatPearls Publishing; 2024. Accessed February 1, 20256. (Online book chapter)
Subscribe to get the full list of 85 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: children with medical complexity, youth with special healthcare needs, medically fragile, complex care, technology dependence, tracheostomy, feeding tube, gastrostomy tube, G tube, gastrojejunostomy tube, GJ tube, cerebrospinal fluid shunt, CSF shunt, ventriculoperitoneal shunt, stoma, tracheostomy stoma complications, feeding tube stoma complications, obstruction, dislodgement, stomal bleeding, stomal infection, granulation, granulation tissue, shunt breakage, shunt reprogramming, shunt infection, cerebrospinal fluid pseudocyst









 678-366-7933
678-366-7933
